5 Childbirth and the Newborn
Meredith Palm
Learning Objectives
- Describe various approaches to childbirth
- Describe a typical vaginal and cesarean delivery, including the stages of childbirth
- Describe two common procedures to assess the condition of the newborn.
- Describe problems newborns experience before, during, and after birth.
- Explain the merits of breastfeeding
- Discuss the importance of nutrition to early physical growth, including nutritional concerns for infants and toddlers
What comes to your mind when you think about birth? Some may describe it as beautiful, a miracle, and a rite of passage. Others may think of pain, fear, and discomfort. Labor and delivery are not easy feats. It is called labor after all because it is a lot of work! In this section, you’ll learn more about the various approaches to childbirth as well as the actual process.
5.1 Approaches to Childbirth

Prepared childbirth refers to being not only physically in good condition to help provide a healthy environment for the baby to develop, but also helping a couple to prepare to accept their new roles as parents and to get information and training that will assist them for delivery and life with the baby as much as possible. The more a couple can learn about childbirth and the newborn, the better prepared they will be for the adjustment they must make to a new life. Nothing can prepare a couple for this completely. Once a couple finds that they are to have a child, they begin to conjure up images of what they think the experience will involve. Once the child is born, they must reconcile those images with reality (Galinsky, 1987). Knowing more of what to expect does help them in forming more realistic images thus making the adjustment easier. Let’s explore some of the methods of prepared childbirth.
HypnoBirthing
Grantley Dick-Read was an English obstetrician and pioneer of prepared childbirth in the 1930s. In his book Childbirth Without Fear, he suggests that the fear of childbirth increases tension and makes the process of childbearing more painful. He believed that if mothers were educated, the fear and tension would be reduced and the need for medication could frequently be eliminated. The Dick-Read method emphasized the use of relaxation and proper breathing with contractions as well as family support and education. Today this method is known as the Mongan Method or HypnoBirthing. Birthing people using this method report feeling like they are lost in a daydream, but focused and in control.
The Lamaze Method
This method originated in Russia and was brought to the United States in the 1950s by Fernand Lamaze. The emphasis of this method is on teaching the birthing person to be in control in the process of delivery. It includes learning muscle relaxation, breathing through contractions, having a focal point (usually a picture to look at) during contractions and having a support person who goes through the training process with the birthing person and serves as a coach during delivery. The Lamaze Method is still the most commonly taught method in the U.S. today.
The Bradley Method
This method originated in the late 1940’s and helps birthing people deliver naturally, with few or no drugs. There are a series of courses that emphasize excellent nutrition and exercise, relaxation techniques to manage pain, and the involvement of the partner as a coach. Parents-to-be are taught to be knowledgeable consumers of birth services and to take responsibility in making informed decisions regarding procedures, attendants and the birthplace. In turn, this will lead to keeping birthing people healthy and low-risk in order to avoid complications that may lead to medical intervention.
Nurse Midwives
Historically in the United States, most babies were born under the care of lay midwives. In the 1920s, middle-class women were increasingly using doctors to assist with childbirth but rural women were still being assisted by lay midwives. The nursing profession began educating nurse-midwives to assist these women. Nurse-midwives continued to assist most rural women with delivery until the 1970s and 1980s when their growth is thought to have posed a threat to the medical profession (Weitz, 2007). Birthing people who are at low risk for birth complications can successfully deliver under the care of nurse-midwives. Some hospitals give privileges to nurse-midwives to deliver there. They may also deliver babies at home or in birthing centers.
Home Birth
Because one out of every 20 births involves a complication, most medical professionals recommend that delivery take place in a hospital. However, some couples choose to have their baby at home. About 1 percent of births occur outside of a hospital in the United States. Two-thirds of these are home births and more than half of these are assisted by midwives. In the United States, birthing people who have had previous children, who are over 25 and who are white are most likely to not give birth in a hospital (MacDorman et al., 2010).
Birthing Centers
A birthing center presents a more home-like environment than a hospital labor ward, typically with more options during labor: food/drink, music, and the attendance of family and friends if desired. Other characteristics can also include non-institutional furniture such as queen-sized beds, large enough for both parents and perhaps birthing tubs or showers for water births. The decor is meant to emphasize the normality of birth. In a birth center, birthing people are free to act more spontaneously during their birth, such as squatting, walking or performing other postures that assist in labor. Active birth is encouraged. The length of stay after a birth is shorter at a birth center; sometimes just 6 hours after birth the birthing parent and infant can go home. One-third of out-of-hospital births occur in freestanding clinics, birthing centers, or in physicians offices or other locations.
Water Birth
Laboring and/or giving birth in a warm tub of water can help a birthing parent relax. The buoyancy of the water can help alleviate discomfort and pressure. Many hospitals have birthing tubs that allow birthing people to labor in them. However, only some hospitals allow for the birth to take place in the water. Some believe that water birth gives a more calm and tranquil transition for the baby from the womb. Water births are more common to occur at home or in birthing centers.
Watch It
Watch this family’s approach to childbirth by having a water birth in their home with a midwife and a doula. Note that there is no audio in the video, only background music.
Not many pregnancies or births go exactly as planned, as seen in the following story of this mother who had to quickly deliver her baby at 30 weeks.
You can view the transcript for “My High-Risk Birth Story | CBC Parents” here (opens in new window).
Hospital Birth
Most births in the U.S. occur in hospitals. Birthing people have the choice to have a medicated or unmedicated delivery. Some do fine with “natural methods” of pain relief alone. Many birthing people blend “natural methods” with medications and medical interventions that relieve pain. Building a positive outlook on childbirth and managing fear may also help some birthing people cope with the pain. Labor pain is not like pain due to illness or injury. Instead, it is caused by contractions of the uterus that are pushing the baby down and out of the birth canal. In other words, labor pain has a purpose.
The most common pain relief method used during labor and delivery is an epidural. An epidural is a procedure that involves placing a tube into the lower back, into a small space outside the spinal cord. Small doses of medicine can be given through the tube as needed throughout labor. With an epidural, pain relief starts 10 to 20 minutes after the medicine has been given. The degree of numbness felt can be adjusted. An epidural can prolong the first and second stages of labor. If given late in labor or if too much medicine is used, it might be hard to push when the time comes.
Watch It
What are the advantages and disadvantages of receiving an epidural? Watch this video to see how the procedure is done.
You can view the transcript for “Epidural Anaesthesia” here (opens in new window).
Another form of pharmacologic pain relief available for laboring people is inhaled nitrous oxide. This is typically a 50/50 mixture of nitrous oxide with air that is an inhaled analgesic and anesthetic. Nitrous oxide has been used for pain management in childbirth since the late 1800’s. The use of inhaled analgesia is commonly used in the UK, Finland, Australia, Singapore, and New Zealand, and is gaining in popularity in the United States..
5.2 The Process of Delivery

The first stage of labor is typically the longest. The First Stage of labor begins with uterine contractions that may initially last about 30 seconds and be spaced 15 to 20 minutes apart. These increase in duration and frequency to more than a minute in length and about 3 to 4 minutes apart. Typically, doctors advise that they should be called when contractions are coming about every 5 minutes. Some birthing people experience false labor or Braxton-Hicks contractions, especially with the first child. These may come and go. They tend to diminish when the birthing person begins walking around. Real labor pains tend to increase with walking.
During this stage, the cervix or opening to the uterus dilates to 10 centimeters or just under 4 inches. This may take around 12-16 hours for first children or about 6-9 hours for people who have previously given birth. Some people (one person in 9) may take over 24 hours to dilate completely. Labor may also begin with a discharge of blood or amniotic fluid. If the amniotic sack breaks, which happens for one out of eight pregnancies, labor will be induced if necessary to reduce the risk of infection.
The second stage involves the passage of the baby through the birth canal. This stage takes about 10-40 minutes. Contractions usually come about every 2-3 minutes. The birthing person pushes and relaxes as directed by the medical staff. Normally the head is delivered first. The baby is then rotated so that one shoulder can come through and then the other shoulder. The rest of the baby quickly passes through. The baby’s mouth and nose are suctioned out. The umbilical cord is clamped and cut.
The third stage is generally less painful, at least when compared to the other stages. During this stage, the placenta or afterbirth is delivered. This typically occurs within 20 minutes after the delivery of the baby. If tearing of the vagina occurred during birth, the tear may be stitched at this time.
Cesarean Section
Cesarean section, also known as C-section, or cesarean delivery, is the use of surgery to deliver babies. A cesarean section is often necessary when a vaginal delivery would put the baby or birthing parent at risk. This may include obstructed labor, twin pregnancy, high blood pressure in the birthing person, breech birth, or problems with the placenta or umbilical cord. Cesarean delivery may be performed based upon the shape of the birthing person’s pelvis or history of a previous C-section. A trial of vaginal birth after C-section may be possible. The World Health Organization recommends that cesarean sections be performed only when medically necessary. Some C-sections are performed without a medical reason, upon request by someone, usually the birthing person.
Watch It
Watch an animation of labor and a vaginal birth.
Watch an animation of a cesarean birth.
5.3 The Newborn and Assessing the Neonate
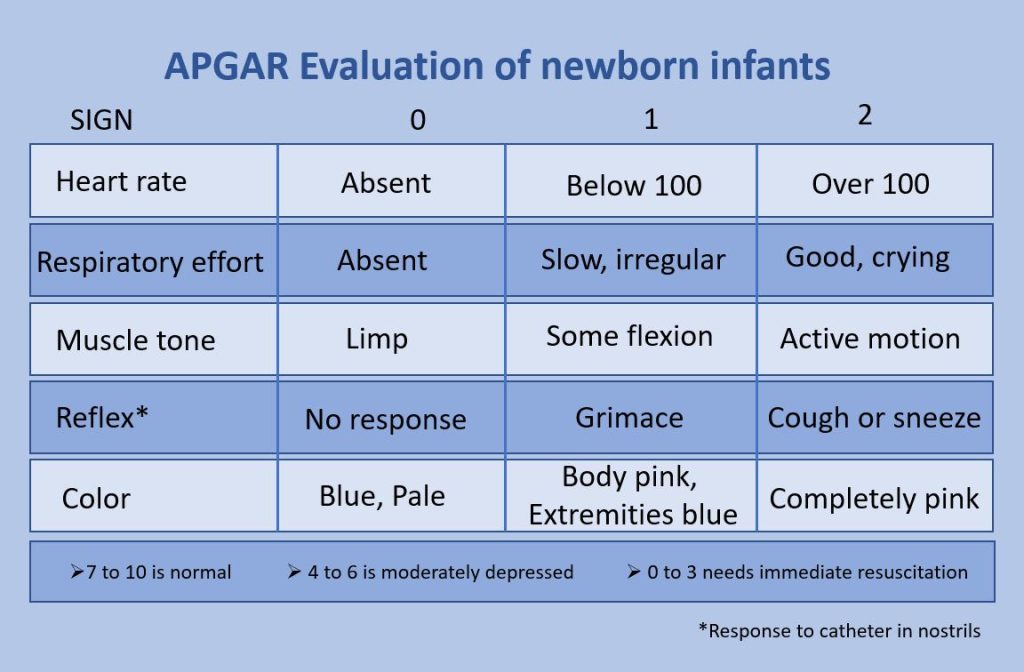
The Apgar assessment is conducted between one minute and five minutes after birth. This is a very quick way to assess the newborn’s overall condition. Five measures are assessed: Heart rate, respiration, muscle tone (assessed by touching the baby’s palm), reflex response (the Babinski reflex is tested), and color. A score of 0 to 2 is given on each feature examined. An Apgar of 5 or less is cause for concern. The second Apgar should indicate improvement with a higher score (see image below).
The APGAR is a common way of assessing the newborn immediately following birth.
Another way to assess the condition of the newborn is the Neonatal Behavioral Assessment Scale (NBAS). The baby’s motor development, muscle tone, and stress response are assessed. This tool has been used around the world to further assess newborns, especially those with low Apgar scores, and to make comparisons of infants in different cultures (Brazelton & Nugent, 1995).
5.4 Problems of the Newborn

Anoxia
Anoxia is a temporary lack of oxygen to the brain. Difficulty during delivery may lead to anoxia which can result in brain damage or in severe cases, death. Babies who suffer both low birth weight and anoxia are more likely to suffer learning disabilities later in life as well.
Low-birth-weight
We previously discussed several teratogens associated with low birth weight such as alcohol, tobacco, and so on. A child is considered low birth weight if he or she weighs less than 5 pounds 8 ounces (2500 grams). About 8.2 percent of babies born in the United States are of low birth weight (Center for Disease Control, 2015a). A low-birth-weight baby has difficulty maintaining adequate body temperature because it lacks the fat that would otherwise provide insulation. Such babies are also at more risk for infection, and 67 percent of these babies are also preterm which can increase their risk for respiratory infection. Very low birth weight babies (2 pounds or less) have an increased risk of developing cerebral palsy.
Additionally, Pettersson et al. (2019) analyzed fetal growth and found that reduced birth weight was correlated with a small, but significant increase in several psychiatric disorders in adulthood. These include attention-deficit/hyperactivity disorder, autism, depression, and obsessive-compulsive disorder. Pettersson et al. theorized that “reduced fetal growth compromises brain development during a critical period, which in turn slightly increases the risk not only for neurodevelopmental disorders but also for virtually all mental health conditions” (p. 540). An insufficient supply of oxygen and nutrients for the developing fetus is proposed as factors that increase the risk for neurodevelopmental disorders.
Preterm
A newborn might also have a low birth weight if it is born at less than 37 weeks gestation, which qualifies it as a preterm baby (CDC, 2015). Early birth can be triggered by anything that disrupts the mother’s system. For instance, vaginal infections can lead to premature birth because such infection causes the mother to release anti-inflammatory chemicals which, in turn, can trigger contractions. Smoking and the use of other teratogens can lead to preterm birth. The earlier a woman quits smoking, the lower the chance that the baby will be born preterm (Someji & Beltrán-Sánchez, 2019). A significant consequence of preterm birth includes respiratory distress syndrome, which is characterized by weak and irregular breathing (United States National Library of Medicine, 2015b).

Saybie (name given to her by the hospital), a baby girl born in San Diego, California is now considered the world’s smallest baby ever to survive (Chiu, 2019). She was born in December 2018 at 23 weeks and 3 days weighing only 8.6 ounces (same size as an apple). After five months in the hospital, Saybie went home in May 2019 weighing 5 pounds.
Small-for-date Infants
Infants that have birth weights that are below expectation based on their gestational age are referred to as small-for-date. These infants may be full-term or preterm, but still weigh less than 90% of all babies of the same gestational age. This is a very serious situation for newborns as their growth is adversely affected. Regev et al. (2003) found that small-for-date infants died at rates more than four times higher than other infants. Remember that many causes of low birth weight and preterm births are preventable with proper prenatal care.
5.5 Newborn Reflexes
Newborns are equipped with several reflexes which are involuntary movements in response to stimulation (see table below). Some of the more common reflexes, such as the sucking reflex and rooting reflex, are important to feeding. The grasping and stepping reflexes are eventually replaced by more voluntary behaviors. Within the first few months of life, these reflexes disappear, while other reflexes, such as the eye-blink, swallowing, sneezing, gagging, and withdrawal reflexes stay with us as they continue to serve important functions. Reflexes offer pediatricians insight into the maturation and health of the nervous system. In preterm infants and those with neurological impairments, some of these reflexes may be absent at birth. Once present, they may persist longer than in a neurologically healthy infant (El-Dib et al., 2012). Reflexes that persist longer than they should can impede normal development (Berne, 2006).
Common Infant Reflexes
| Reflex | Description | Image |
|---|---|---|
| Sucking | Suck on anything that touches the lips. |  |
| Rooting | Turning the head when the cheek is touched. |  |
| Grasp | Fingers automatically grip anything that touches the palm of the hand. |  |
| Babinski | The toes will fan out and curl when the sole of the foot is stroked from heel to toe. |  |
| Moro | A sudden noise or loss of support to the head will cause infants to spread out their arms and legs and then quickly contract the limbs inward. |  |
| Tonic Neck | When lying on the back with the head to one side infants will extend the arm and leg on that side while flexing the limbs on the opposite side (looks like a fencer pose). |  |
| Stepping | Legs move in a stepping-like motion when feet touch a smooth surface. |  |
5.6 Infant Growth and Nutrition
Good nutrition in a supportive environment is vital for an infant’s healthy growth and development. Remember, from birth to 1 year, infants triple their weight and increase their height by half, and this growth requires good nutrition. For the first 6 months, babies are fed breast milk or formula. Starting good nutrition practices early can help children develop healthy dietary patterns. Infants need to receive nutrients to fuel their rapid physical growth. Malnutrition during infancy can result in not only physical but also cognitive and social consequences. Without proper nutrition, infants cannot reach their physical potential.
Benefits of Breastfeeding
Breast milk is considered the ideal diet for newborns due to the nutritional makeup of the colostrum and subsequent breast milk production. Colostrum, the milk produced during pregnancy and just after birth, has been described as “liquid gold.” Colostrum is packed with nutrients and other important substances that help the infant build up their immune system. Most babies will get all the nutrition they need through colostrum during the first few days of life (CDC, 2018).[1] Breast milk changes by the third to fifth day after birth, becoming much thinner but containing just the right amount of fat, sugar, water, and proteins to support overall physical and neurological development. It provides a source of iron more easily absorbed in the body than the iron found in dietary supplements, it provides resistance against many diseases, it is more easily digested by infants than formula, and it helps babies make a transition to solid foods more easily than if bottle-fed.
The reason infants need such a high fat content is the process of myelination which requires fat to insulate the neurons. There has been some research, including meta-analyses, to show that breastfeeding is connected to advantages with cognitive development (Anderson et al. 1999)[2]. Low birth-weight infants had greater benefits from breastfeeding than did normal-weight infants in a meta-analysis of twenty controlled studies examining the overall impact of breastfeeding (Anderson et al., 1999). This meta-analysis showed that breastfeeding may provide nutrients required for rapid development of the immature brain and be connected to more rapid or better development of neurologic function. The studies also showed that a longer duration of breastfeeding was accompanied by greater differences in cognitive development between breastfed and formula-fed children. Whereas normal-weight infants showed a 2.66-point difference, low-birth-weight infants showed a 5.18-point difference in IQ compared with weight-matched, formula-fed infants (Anderson et al, 1999). These studies suggest that nutrients present in breast milk may have a significant effect on neurologic development in both premature and full-term infants.
For most babies, breast milk is also easier to digest than formula. Formula-fed infants experience more diarrhea and upset stomachs. The absence of antibodies in the formula often results in a higher rate of ear infections and respiratory infections. Children who are breastfed have lower rates of childhood leukemia, asthma, obesity, type 1 and 2 diabetes, and a lower risk of SIDS. For all of these reasons, it is recommended that mothers breastfeed their infants until at least 6 months of age and that breast milk be used in the diet throughout the first year (U.S. Department of Health and Human Services, 2004a in Berk, 2007).
Several recent studies have reported that it is not just babies that benefit from breastfeeding. Breastfeeding stimulates contractions in the uterus to help it regain its normal size, and women who breastfeed are more likely to space their pregnancies farther apart. Mothers who breastfeed are at lower risk of developing breast cancer, especially among higher-risk racial and ethnic groups (Islami et al., 2015).[3] Other studies suggest that women who breastfeed have lower rates of ovarian cancer (Titus-Ernstoff et al., 2010)[4], and reduced risk for developing Type 2 diabetes (Gunderson, et al., 2015)[5], and rheumatoid arthritis (Karlson et al., 2004).[6]
As of 2022, the recommendation from the American Academy of Pediatrics is that breastfeeding is the only source of nutrition for an infant for the first six months of life and that breastfeeding should be supported for two years or beyond (Meek & Noble, 2022) Most mothers who breastfeed in the United States stop breastfeeding at about 6-8 weeks, often to return to work outside the home (United States Department of Health and Human Services (USDHHS), 2011) [7]. Mothers can certainly continue to provide breast milk to their babies by expressing and freezing the milk to be bottle fed at a later time or by being available to their infants at feeding time, but some mothers find that after the initial encouragement they receive in the hospital to breastfeed, the outside world is less supportive of such efforts. Some workplaces support breastfeeding mothers by providing flexible schedules and welcoming infants, but many do not. And the public support of breastfeeding is sometimes lacking.
The Providing Urgent Maternal Protections (PUMP) for Nursing Mothers Act was signed into law in December 2022, requiring employers to provide break time and a private place to express breastmilk and expanding existing protections to an additional nine million employees (U.S. Department of Labor, 2023). It has yet to be determined the extent to which these protections improve breastfeeding rates in the United States. Women in Canada are more likely to breastfeed than those in the United States, and the Canadian health recommendation is for breastfeeding to continue until 2 years of age. Facilities in public places in Canada such as malls, ferries, and workplaces provide more support and comfort for the breastfeeding mother and child than found in the United States.
In addition to the nutritional and health benefits of breastfeeding, breast milk is free! Anyone who has priced formula recently can appreciate this added incentive to breastfeeding. Prices for a month’s worth of formula can easily range from $130-$200. Prices for a year’s worth of formula and feeding supplies can cost well over $1,500 (USDHHS, 2011). One reason for high formula costs is a low supply of the product combined with high consumer demand. Supply chain issues decreased the availability of infant formula leading to a severe, acute shortage in May 2022 (Abrams & Duggan, 2022) that subsequently increased the frequency of unsafe infant feeding practices among parents desperate to feed their infants (Cernioglo & Smilowitz, 2023).
When Breastfeeding Doesn’t Work
There are occasions when mothers may be unable to breastfeed babies, often for a variety of health, social, and emotional reasons. For example, breastfeeding generally does not work:
- when the baby is adopted or born via a surrogate who is unavailable to breastfeed
- when the biological mother has a transmissible disease such as tuberculosis or HIV
- when the mother is addicted to drugs or taking any medication that may be harmful to the baby (including some types of birth control)
- when the infant was born to (or adopted by) a family with two fathers and the surrogate mother is not available to breastfeed
- when there are attachment issues between mother and baby
- when the mother or the baby is in the Intensive Care Unit (ICU) after the delivery process
- when the baby and mother are attached but the mother does not produce enough breast milk
One early argument given to promote the practice of breastfeeding (when health issues are not the case) is that it promotes bonding and healthy emotional development for infants. However, this does not seem to be a unique case. Breastfed and bottle-fed infants adjust equally well emotionally (Ferguson & Woodward, 1999). This is good news for mothers who may be unable to breastfeed for a variety of reasons and for fathers who might feel left out as a result.
Global Considerations and Malnutrition
In the 1960s, formula companies led campaigns in developing countries to encourage mothers to feed their babies on infant formula. Many mothers felt that formula would be superior to breast milk and began using formula. The use of formula can certainly be healthy under conditions in which there is adequate, clean water with which to mix the formula and adequate means to sanitize bottles and nipples. However, in many of these countries, such conditions were not available, and babies often were given diluted, contaminated formula which made them become sick with diarrhea and become dehydrated. These conditions continue today and now many hospitals prohibit the distribution of formula samples to new mothers in efforts to get them to rely on breastfeeding. Many of these mothers do not understand the benefits of breastfeeding and have to be encouraged and supported in order to promote this practice.
The World Health Organization (2018) recommends:
- initiation of breastfeeding within one hour of birth
- exclusive breastfeeding for the first six months of life
- introduction of solid foods at six months together with continued breastfeeding up to two years of age or beyond
Children in developing countries and countries experiencing the harsh conditions of war are at risk for two major types of malnutrition. Infantile marasmus refers to starvation due to a lack of calories and protein. Children who do not receive adequate nutrition lose fat and muscle until their bodies can no longer function. Babies who are breastfed are much less at risk of malnutrition than those who are bottle-fed. After weaning, children who have diets deficient in protein may experience kwashiorkor, or the “disease of the displaced child,” often occurring after another child has been born and taken over breastfeeding. This results in a loss of appetite and swelling of the abdomen as the body begins to break down the vital organs as a source of protein.
Licenses & Attributions (Click to expand)
CC Licensed Content
- “Childbirth.” Authored by: Julie Lazzara for Lumen Learning. Provided by: Lumen Learning. Located at: https://courses.lumenlearning.com/wm-lifespandevelopment/chapter/childbirth/. License: CC BY: Attribution
- Psyc 200 Lifespan Psychology. Authored by: Laura Overstreet. Located at: http://opencourselibrary.org/econ-201/. License: CC BY: Attribution
- Authored by: OpenStax College. Located at: https://en.wikipedia.org/wiki/Childbirth#/media/File:2920_Stages_of_Childbirth-02.jpg. License: CC BY: Attribution. License Terms: Download for free at http://cnx.org/contents/FPtK1zmh@6.27:zMTtFGyH@4/Introduction
- Bradley Method of natural childbirth. Provided by: Wikipedia. Located at: https://en.wikipedia.org/wiki/Bradley_method_of_natural_childbirth. License: CC BY-SA: Attribution-ShareAlike
- Caesarean section. Provided by: Wikipedia. Located at: https://en.wikipedia.org/wiki/Caesarean_section. License: CC BY-SA: Attribution-ShareAlike
All Rights Reserved Content
- My High-Risk Birth Story. Provided by: CBC Parents. Located at: https://www.youtube.com/watch?time_continue=88&v=jzBQQXy5XRE. License: Other. License Terms: Standard YouTube License
- Home Birth Water Birth with Doula and Midwife. Provided by: Yema Mamas. Located at: https://www.youtube.com/watch?v=wczscWXk8e4. License: Other. License Terms: Standard YouTube License
- Epidural Anaesthesia. Authored by: LHSCCanada. Located at: https://www.youtube.com/watch?v=2tw-SXI3wKU. License: Other. License Terms: Standard YouTube License
Public Domain Content
- Couple in baby class. Authored by: Senior Airman Krystal Ardrey. Provided by: U.S. Air Force. Located at: https://www.airforcemedicine.af.mil/News/Photos/igphoto/2001602805/. License: Public Domain: No Known Copyright
References
Abrams, S. A., & Duggan, C. P. (2022). Infant and child formula shortages: Now is the time to prevent recurrences. The American Journal of Clinical Nutrition, 116(2), 289-292.
Anderson, J.W., Johnstone, B.M., & Remley, D.T. (1999). Breast-feeding and cognitive development: A meta-analysis. The American Journal of Clinical Nutrition, 70(4), 525-535. https://doi.org/10.1093/ajcn/70.4.525
Berne, S. A. (2006). The primitive reflexes: Considerations in the infant. Optometry & Vision Development, 37(3), 139-145.
Brazelton, T. B., & Nugent, J. K. (1995). Neonatal behavioral assessment scale. Mac Keith Press.
Centers for Disease Control and Prevention. (2015). Preterm birth. http://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm
Centers for Disease Control and Prevention. (2018). What to expect while breastfeeding. https://www.cdc.gov/nutrition/InfantandToddlerNutrition/breastfeeding/what-to-expect.html
Cernioglo, K., & Smilowitz, J. T. (2023). Infant feeding practices and parental perceptions during the 2022 United States infant formula shortage crisis. BMC pediatrics, 23(1), 320.
Chiu, A. (2019, May 30). ‘She’s a miracle’: Born weighing about as much as ‘a large apple,’ Saybie is the world’s smallest surviving baby. The Washington Post. https://www.washingtonpost.com/nation/2019/05/30/world-smallest-surviving-baby-saybie-miracle/?noredirect=on&utm_term=.7c8d0bb6acf7
El-Dib, M., Massaro, A. N., Glass, P., & Aly, H. (2012). Neurobehavioral assessment as a predictor of neurodevelopmental outcome in preterm infants. Journal of Perinatology, 32(4), 299-303.
Fergusson, D. M., & Woodward, L. J. (1999). Maternal age and educational and psychosocial outcomes in early adulthood. The Journal of Child Psychology and Psychiatry and Allied Disciplines, 40, 479-489.
Giving birth naturally: Natural childbirth techniques. (n.d.). American Pregnancy Association. http://americanpregnancy.org/labor-and-birth/natural-childbirth-techniques/ ↵
Gunderson, E.P., Hurston, S.R., Dewey, K.G., Faith, M.S., Charvat-Aguilar, N., Khoury, V. C., Nguyen, V.T., & Quesenberry, C.P. (2015). The study of women, infant feeding and type 2 diabetes after GDM pregnancy and growth of their offspring (SWIFT Offspring study): Prospective design, methodology and baseline characteristics. BMC Pregnancy and Childbirth, 15, 150. https://doi.org/10.1186/s12884-015-0587-z
Islami, F., Liu, Y., Jemal, A., Zhou, J., Weiderpass, E., Colditz, G., Boffetta, P., & Weiss, M. (2015). Breastfeeding and breast cancer risks by receptor status- a systematic review and meta-analysis. Annals of Oncology, 26(12), 2398–2407
Karlson, E.W., Mandl, L.A., Hankinson, S. E., & Grodstein, F. (2004). Do breast-feeding and other reproductive factors influence future risk of rheumatoid arthritis? Results from the Nurses’ Health Study. Arthritis Rheumatology, 50(11), 3458-67.
Meek, J. Y., Noble, L., & Section on Breastfeeding. (2022). Policy statement: breastfeeding and the use of human milk. Pediatrics, 150(1).
Pettersson, E., Larsson, H., D’Onofrio, B., Almqvist, C., & Lichtenstein, P. (2019). Association of fetal growth with general and specific mental health conditions. JAMA Psychiatry, 76(5), 536-543.
Regev, R.H., Lusky, T. Dolfin, I. Litmanovitz, S. Arnon, B. & Reichman. (2003). Excess mortality and morbidity among small-for-gestational-age premature infants: A population based study. Journal of Pediatrics, 143, 186-191.
Someji, S., & Beltrán-Sánchez, H. (2019). Association of maternal cigarette smoking and smoking cessation with preterm birth. JAMA Network Open, 2(4), doi: 10.1001/jamanetworkopen.2019.2514
Titus-Ernstoff, Rees, L. Terry, R.R., & Cramer, D. W. (2010). Breast-feeding the last born child and risk of ovarian cancer. Cancer Causes Control, 21(2), 201–207.
United States Department of Health and Human Services, Office of Women’s Health. (2011). Your guide to breastfeeding. Washington D.C.
United States Department of Labor. (2022). FLSA Protections to pump at work. https://www.dol.gov/agencies/whd/pump-at-work
United States National Library of Medicine. (2015b). Neonatal respiratory distress syndrome. https://medlineplus.gov/ency/article/001563.htm
World Health Organization. (2018). Breastfeeding. https://www.who.int/health-topics/breastfeeding#tab=tab_2
Media Attributions
- APGAR_score-1024×672-1
- Human_Infant_in_Incubator-300×202-1
- Sucking
- Rooting
- Grasping
- Babinski
- Moro
- Tonic Neck
- Stepping
