4 Prenatal Development
Learning Objectives
- Differentiate between development during the germinal, embryonic, and fetal periods
- Explain the process of brain development during the prenatal period
- Define teratogens and explain how various factors influence their effects
- Explain maternal and paternal factors that affect the developing fetus
- Identify the types of prenatal assessment
- Explain potential complications of pregnancy and delivery
How did you come to be who you are? From beginning as a one-cell structure to your birth, prenatal development occurs in an orderly and delicate sequence. There are three stages of prenatal development: germinal, embryonic, and fetal. Keep in mind that this is different than the three trimesters of pregnancy. Let’s look at what happens to the developing baby in each of these stages.
4.1 Periods of Prenatal Development
You may be familiar with the three trimesters of pregnancy, three trimesters consisting of three months each to equal the entire pregnancy of nine months. People who have recently given birth frequently refer to how they felt during their first, second, or third trimester, and this is easy to do, as the trimesters generally describe the experience of the gestational parent during these three temporally equal intervals of pregnancy. When we look at the development of the organism from zygote to fetus to newly born infant, we also examine three periods of development. However, these periods are not equal in length, and they do not align with the gestational parent’s experience of the three trimesters. Actually, a full-term pregnancy is considered to be 40 weeks long (which would be equivalent to 10, not nine, months!), and two of the three periods of development occur within the first trimester. Let’s take a look at some of the changes that take place during each of the three periods of prenatal development: the germinal period, the embryonic period, and the fetal period.
The Germinal Period (Weeks 1-2)
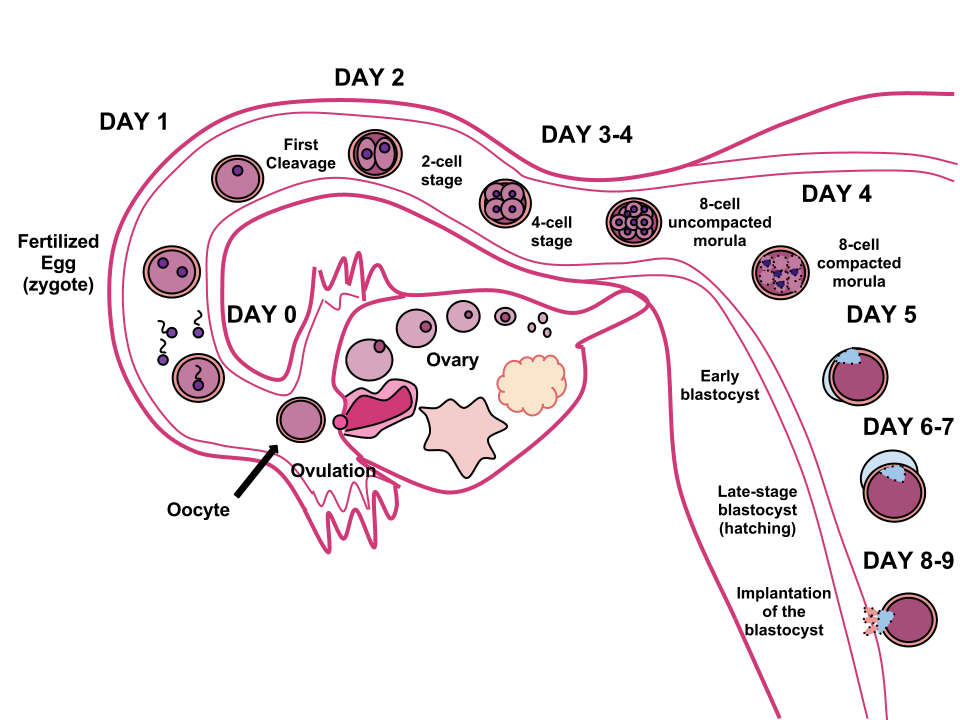
The germinal period (about 14 days in length) lasts from conception to implantation of the fertilized egg in the lining of the uterus (see Figure 5.3). At ejaculation, millions of sperm are released into the vagina, but only a few reach the egg and typically only one fertilizes the egg. Once a single sperm has entered the wall of the egg, the wall becomes hard and prevents other sperm from entering. After the sperm has entered the egg, the tail of the sperm breaks off and the head of the sperm, containing the genetic information from the father, unites with the nucleus of the egg. The egg is typically fertilized in the top section of the fallopian tube and continues its journey to the uterus. As a result, a new cell is formed. This cell, containing the combined genetic information from both parents, is referred to as a zygote.
During this time, the organism begins cell division through mitosis. After five days of mitosis, there is a group of 100 cells, which is now called a blastocyst. The blastocyst consists of both an inner and outer group of cells. The inner group of cells, or embryonic disk will become the embryo, while the outer group of cells, or trophoblast, becomes the support system that nourishes the developing organism. This stage ends when the blastocyst fully implants into the uterine wall (U.S. National Library of Medicine, 2015). Approximately 50-75% of blastocysts do not implant in the uterine wall (Betts et al., 2019).
Mitosis is a fragile process and fewer than half of all zygotes survive beyond the first two weeks (Hall, 2004). Some of the reasons for this include the egg and sperm not joining properly, meaning that their genetic material does not combine; there is too little or damaged genetic material; the zygote does not replicate; or the blastocyst does not implant into the uterine wall. The failure rate is higher for in vitro conceptions. The image below illustrates the journey of the ova from its release to its fertilization, cell duplication, and implantation into the uterine lining.
Infertility
Infertility is the inability to conceive a child or carry a child to birth and is usually defined when an individual has not had a successful pregnancy after one year of trying to conceive. About 75 percent of the causes of infertility can be identified; these include diseases, such as sexually transmitted diseases that can cause scarring of the reproductive tubes in males or females, or developmental problems frequently related to abnormal hormone levels in one of the individuals. Inadequate nutrition, especially starvation, can delay menstruation. Stress can also lead to infertility. Short-term stress can affect hormone levels, while long-term stress can delay puberty and cause less frequent menstrual cycles. Other factors that affect fertility include toxins (such as cadmium), tobacco smoking, marijuana use, gonadal injuries, and aging.
If infertility is identified, several assisted reproductive technologies (ART) are available to aid conception. A common type of ART is in vitro fertilization (IVF) where an egg and sperm are combined outside the body and then placed in the uterus. This technique was first successfully performed in mice by Anne McLaren and John Biggers, whose work is credited as among the most significant in reproductive medicine. Eggs are obtained after extensive hormonal treatments that prepare mature eggs for fertilization and prepare the uterus for implantation of the fertilized egg. Sperm are obtained, combined with the eggs, and supported through several cell divisions to ensure the viability of the zygotes. When the embryos have reached the eight-cell stage, one or more are implanted into the gestational parent’s or carrier’s uterus. If fertilization is not accomplished by simple IVF, a procedure that injects the sperm into an egg can be used. This is called intracytoplasmic sperm injection (ICSI) and is shown in the image above. IVF procedures produce a surplus of fertilized eggs and embryos that can be frozen and stored for future use. The procedures can also result in multiple births.
The Embryonic Period (Weeks 3-8)

Starting the third week the blastocyst has implanted in the uterine wall. Upon implantation, this multi-cellular organism is called an embryo. Now blood vessels grow, forming the placenta. The placenta is a structure connected to the uterus that provides nourishment and oxygen from the mother to the developing embryo via the umbilical cord. During this period, cells continue to differentiate. Growth during prenatal development occurs in two major directions: from head to tail called cephalocaudal development and from the midline outward referred to as proximodistal development. This means that those structures nearest the head develop before those nearest the feet and those structures nearest the torso develop before those away from the center of the body (such as hands and fingers). The head develops in the fourth week and the precursor to the heart begins to pulse. In the early stages of the embryonic period, gills and a tail are apparent. However, by the end of this stage, they disappear, and the organism takes on a more human appearance. Some organisms fail during the embryonic period, usually due to gross chromosomal abnormalities. As in the case of the germinal period, often the gestational parent does not yet know that they are pregnant.
It is during this stage that the major structures of the body are taking form making the embryonic period the time when the organism is most vulnerable to the greatest amount of damage if exposed to harmful substances. Gestational parents are not often aware of the risks they introduce to the developing embryo during this time. The embryo is approximately 1 inch in length and weighs about 8 grams at the end of eight weeks (Betts et al., 2019). The embryo can move and respond to touch at this time.
The Fetal Period (Weeks 9-40)
From the ninth week until birth, the organism is referred to as a fetus. During this stage, the major structures are continuing to develop. By the 12th week, the fetus has all its body parts including external genitalia. In the following weeks, the fetus will develop hair, nails, and teeth and the excretory and digestive systems will continue to develop. The fetus is about 3 inches long and weighs about 28 grams.
During the 4th – 6th months, the eyes become more sensitive to light and hearing develops. The respiratory system continues to develop, and reflexes such as sucking, swallowing, and hiccupping, develop during the 5th month.
Cycles of sleep and wakefulness are present at this time as well. The first chance of survival outside the womb, known as the age of viability, is reached at about 24 weeks (Morgan et al., 2008). The majority of the neurons in the brain have developed by 24 weeks, although they are still rudimentary, and the glial or nurse cells that support neurons continue to grow. At 24 weeks the fetus can feel pain (Royal College of Obstetricians and Gynecologists, 1997). By the time the fetus reaches this point, it weighs up to 1.4 pounds. The hearing has developed, so the fetus can respond to sounds. The internal organs, such as the lungs, heart, stomach, and intestines, have formed enough that a fetus born prematurely at this point has a chance to survive outside of the gestational parent’s womb.
Between the 7th – 9th months, the fetus is primarily preparing for birth. It is exercising its muscles, and its lungs begin to expand and contract. The fetus gains about 5 pounds and 7 inches during this last trimester of pregnancy, and during the 8th month, a layer of fat develops under the skin. This layer of fat serves as insulation and helps the baby regulate body temperature after birth.
At around 36 weeks the fetus is almost ready for birth. It weighs about 6 pounds and is about 18.5 inches long. By week 37, all the fetus’s organ systems are developed enough that it can survive outside the gestational parent’s uterus without many of the risks associated with premature birth. The fetus continues to gain weight and grow in length until approximately 40 weeks. By then the fetus has very little room to move around and birth becomes imminent. The progression through the stages is shown in the image below.

Prenatal Brain Development
Prenatal brain development begins in the third gestational week with the differentiation of stem cells, which can produce all the different cells that make up the brain (Stiles & Jernigan, 2010). The location of these stem cells in the embryo is referred to as the neural plate. By the end of the third week, two ridges appear along the neural plate first forming the neural groove and then the neural tube. The open region in the center of the neural tube forms the brain’s ventricles and spinal canal. By the end of the embryonic period, or week eight, the neural tube has further differentiated into the forebrain, midbrain, and hindbrain.
Brain development during the fetal period involves neuron production, migration, and differentiation. From the early fetal period until mid-gestation, most of the 85 billion neurons have been generated and many have already migrated to their brain positions. Neurogenesis, or the formation of neurons, is largely completed after five months of gestation. One exception is in the hippocampus, which continues to develop neurons throughout life. Neurons that form the neocortex, or the layer of cells that lie on the surface of the brain, migrate to their location in an orderly way. Neural migration is mostly completed in the cerebral cortex by 24 weeks (Poduri & Volpe, 2018).
Once in position, neurons begin to produce dendrites and axons that begin to form the neural networks responsible for information processing. Regions of the brain that contain the cell bodies are referred to as gray matter because they look gray in appearance. The axons that form the neural pathways make up the white matter because they are covered in myelin, a fatty substance that is white in appearance. Myelin aids in both the insulation and efficiency of neural transmission. Although cell differentiation is complete at birth, the growth of dendrites, axons, and synapses continues for years.
4.2 Environmental Risks Teratology
Good prenatal care is essential for healthy development. The developing child is most at risk for severe problems during the first three months of development. Unfortunately, this is a time when many gestational parents are unaware that they are pregnant. Today, we know many of the factors that can jeopardize the health of the developing child. The study of factors that contribute to birth defects is called teratology. Teratogens are environmental factors that can contribute to birth defects and include some parental diseases, pollutants, drugs, and alcohol.
Factors Influencing Prenatal Risks
There are several considerations in determining the kind and amount of damage that can result from exposure to a particular teratogen (Berger, 2005). These include:
- The timing of the exposure. Structures in the body are vulnerable to the most severe damage when they are forming. If a substance is introduced during a particular structure’s critical period (time of development), the damage to that structure may be greater. For example, the ears and arms reach their critical periods at about 6 weeks after conception. If a gestational parent exposes the embryo to certain substances during this period, its ears and arms may be malformed.
- The amount of exposure. Some substances are not harmful unless the amounts reach a certain level. The critical level depends in part on the size and metabolism of the gestational parent.
- The number of teratogens. Fetuses exposed to multiple teratogens typically have more problems than those exposed to only one.
- Genetics. Genetic make-up also plays a role in the impact a particular teratogen has on a child. This is suggested by research showing that fraternal twins exposed to the same prenatal environment, do not always experience the same teratogenic effects. The genetic makeup of the gestational parent can also have an effect; some gestational parents may be more resistant to teratogenic effects than others.
- Being male or female. Males are more likely to experience damage due to teratogens than females. It is believed that the Y chromosome, which contains fewer genes than the X, may make males more vulnerable.
Alcohol
One of the most common teratogens is alcohol, and because half of all pregnancies in the United States are unplanned, it is recommended that people of child-bearing age take great caution against drinking alcohol when not using birth control or when pregnant (CDC, 2005). Alcohol use during pregnancy is the leading preventable cause of intellectual disabilities in children in the United States (Maier & West, 2001). Alcohol consumption at any point during pregnancy, but particularly during the second month of prenatal development, may lead to neurocognitive and behavioral difficulties that can last a lifetime.
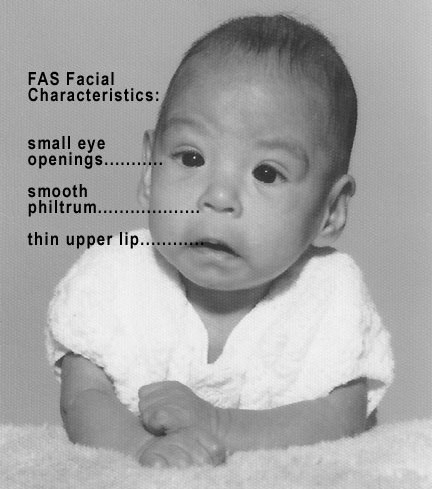
In extreme cases, alcohol consumption during pregnancy can lead to fetal death, but also can result in Fetal Alcohol Spectrum Disorders (FASD), which is an umbrella term for the range of effects that can occur due to alcohol consumption during pregnancy (March of Dimes, 2016a). The most severe form of FASD is Fetal Alcohol Syndrome (FAS). Children with FAS share certain physical features such as flattened noses, small eye holes, and small heads.
Cognitively, these children have poor judgment, poor impulse control, higher rates of ADHD, learning issues, and lower IQ scores. These developmental problems and delays persist into adulthood (Streissguth et al., 1996) and contribute to criminal behavior, psychiatric problems, and unemployment (CDC, 2016a). Based on animal studies, it has been hypothesized that a gestational parent’s alcohol consumption during pregnancy may predispose their child to like alcohol (Youngentob et al., 2007). Binge drinking, or 4 or more drinks in 2 to 3 hours, during pregnancy increases the chance of having a baby with FASD (March of Dimes, 2016a).
Tobacco
Another widely used teratogen is tobacco; in 2016, more than 7% of pregnant women smoked in 2016 (Someji & Beltrán-Sánchez, 2019). According to Tong et al. (2013) in conjunction with the Centers for Disease Control and Prevention, data from 27 sites in 2010 representing 52% of live births, showed that among women with recent live births:
- About 23% reported smoking in the 3 months before pregnancy.
- Almost 11% reported smoking during pregnancy.
- More than half (54.3%) reported that they quit smoking by the last 3 months of pregnancy.
- Almost 16% reported smoking after delivery.
When comparing the ages of women who smoked:
- Women <20, 13.6% smoked during pregnancy
- Women 20–24,17.6% smoked during pregnancy
- Women 25–34, 8.8% smoked during pregnancy
- Women ≥35, 5.7% smoked during pregnancy
The findings among racial and ethnic groups indicated that smoking during pregnancy was highest among American Indians/Alaska Natives (26.0%) and lowest among Asians/Pacific Islanders (2.1%).
When a pregnant person smokes, the fetus is exposed to dangerous chemicals including nicotine, carbon monoxide, and tar, which lessen the amount of oxygen available to the fetus. Oxygen is important for overall growth and development. Tobacco use during pregnancy has been associated with ectopic pregnancy (fertilized egg implants itself outside of the uterus), placenta previa (placenta lies low in the uterus and covers all or part of the cervix), placenta abruption (placenta separates prematurely from the uterine wall), preterm delivery, low birth weight, stillbirth, fetal growth restriction, sudden infant death syndrome (SIDS), birth defects, learning disabilities, and early puberty in girls (Center for Disease Control, 2015d).
When gestational parents are exposed to secondhand smoke during pregnancy, this also increases the risk of low-birth-weight infants. In addition, exposure to thirdhand smoke, or toxins from tobacco smoke that linger on clothing, furniture, and in locations where smoking has occurred, can have a negative impact on infants’ lung development. Rehan et al. (2011) found that prenatal exposure to thirdhand smoke played a greater role in altered lung functioning than postnatal exposure.
Prescription/Over-The-Counter Drugs
About 70% of pregnant people take at least one prescription drug (March of Dimes, 2016e). A person should not be taking any prescription medication during pregnancy unless it was prescribed by a health care provider who knows that person is pregnant. Some prescription drugs can cause birth defects, problems in overall health, and development of the fetus. Over-the-counter drugs are also a concern during the prenatal period because they may cause certain health problems. For example, the pain reliever ibuprofen can cause serious blood flow problems to the fetus during the last three months.
Illicit Drugs
Common illicit drugs include marijuana, cocaine, ecstasy and other club drugs, heroin, and prescription drugs that are abused. It is difficult to fully determine the effects of particular illicit drugs on a developing fetus because most gestational parents who take illicit drugs, frequently take more than one substance and have other unhealthy behaviors. These include smoking, drinking alcohol, not eating healthy meals, and being more likely to get a sexually transmitted disease.
However, several problems seem clear. The use of cocaine is connected with low birth weight, stillbirths, and spontaneous abortion (miscarriage). Heavy marijuana use is associated with problems in brain development (March of Dimes, 2016c). If a baby’s gestational parent used an addictive drug during pregnancy that baby can get addicted to the drug before birth and go through drug withdrawal after birth, also known as Neonatal abstinence syndrome (March of Dimes, 2015d). Other complications of illicit drug use include premature birth, smaller-than-normal head size, birth defects, heart defects, and infections. Additionally, babies born to gestational parents who use drugs may have problems later in life, including death from sudden infant death syndrome, slower than normal growth, and learning and behavior difficulties. Children of substance-using parents are also considered at high risk for a range of biological, developmental, academic, and behavioral problems, including developing substance abuse problems of their own (Conners et al., 2003).
Pollutants
There are more than 83,000 chemicals used in the United States with little information on their effects on unborn children (March of Dimes, 2016b).
- Lead poisoning. An environmental pollutant of significant concern is lead, which has been linked to fertility problems, high blood pressure, low birth weight, prematurity, miscarriage, and delayed neurological development. Grossman and Slutsky (2017) found that babies born in Flint Michigan, an area identified with high lead levels in the drinking water, were premature, weighed less than average, and gained less weight than normal.
- Pesticides. Chemicals in certain pesticides are also potentially damaging and may lead to miscarriage, low birth weight, premature birth, birth defects, and learning problems (March of Dimes, 2014).
- Bisphenol A. Prenatal exposure to bisphenol A (BPA), a chemical commonly used in plastics and food and beverage containers, may disrupt the action of certain genes contributing to particular birth defects (March of Dimes, 2016b).
- Radiation. If a gestational parent is exposed to radiation, it can get into the bloodstream and pass through the umbilical cord to the fetus. Radiation can also build up in body areas close to the uterus, such as the bladder. Radiation exposure can cause result in miscarriage, affect brain development, slow the baby’s growth, or cause birth defects or cancer.
- Mercury. Mercury, a heavy metal, can cause brain damage and affect the baby’s hearing and vision. This is why people are cautioned about the amount and type of fish they consume during pregnancy.
 Toxoplasmosis
Toxoplasmosis
The tiny parasite, toxoplasma gondii, causes an infection called toxoplasmosis. According to the March of Dimes (2012d), toxoplasma gondii infects more than 60 million people in the United States. A healthy immune system can keep the parasite at bay resulting in no symptoms, so most people do not know they are infected. As a routine prenatal screening frequently does not test for the presence of this parasite, pregnant people may want to talk to their health-care provider about being tested. Toxoplasmosis can cause premature birth, and stillbirth, and can result in birth defects to the eyes and brain. While most babies born with this infection show no symptoms, ten percent may experience eye infections, enlarged liver and spleen, jaundice, and pneumonia. To avoid being infected, gestational parents should avoid eating undercooked or raw meat and unwashed fruits and vegetables, touching cooking utensils that touch raw meat or unwashed fruits and vegetables, and touching cat feces, soil, or sand (do not clean the litter box if pregnant). If people think they may have been infected during pregnancy, they should have their newborn tested.
Sexually Transmitted Diseases
Gonorrhea, syphilis, and chlamydia are sexually transmitted infections that can be passed to the fetus by an infected gestational parent. Gestational parents should be tested as early as possible to minimize the risk of spreading these infections to their unborn children. Additionally, the earlier the treatment begins, the better the health outcomes for parents and babies (CDC, 2016d). Sexually transmitted diseases (STDs) can cause ectopic pregnancy, miscarriage, premature rupture of the amniotic sac, premature birth, stillbirths, and birth defects (March of Dimes, 2013). Although some STDs can cross the placenta and infect the developing fetus, most babies become infected with STDS while passing through the birth canal during delivery.
Congenital Syphilis on the Raise Across the United States and Wisconsin
Of particular concern is the continued five-year increase in syphilis cases, showing a staggering 1,450% rise from 2019 and surpassing the national average, directly contributing to a worrisome increase in congenital syphilis cases (31 in 2024, up from 25 in 2023), which can cause stillbirth or severe health problems for newborns. This is a 1,450% increase from 2019! (Wisconsin Department of Health Services, 2025).
Up to 40% of infants infected with congenital syphilis can be stillborn or succumb to the infection, and while syphilis is treatable with antibiotics, untreated cases can result in severe birth defects such as cataracts, deafness, seizures, or even death. Wisconsin State Health Officer Paula Tran emphasizes that while STIs are preventable, many show no symptoms, making timely, accessible testing, treatment with antibiotics, and comprehensive sexual health education crucial for all sexually active individuals, especially those who are pregnant or may become pregnant (WI Department of Health Services, 2025).
For additional information about Syphilis and other STDs, travel to the WI DHS website.
Human Immunodeficiency Virus (HIV)
One of the most potentially devastating teratogens is HIV. One of the main ways children under age 13 become infected with HIV is via mother-to-child transmission of the virus prenatally, during labor, or by breastfeeding (CDC, 2016c). Some measures can be taken to lower the chance the child will contract the disease. HIV-positive gestational parents who take antiviral medications during their pregnancy greatly reduce the chance of passing the virus to the fetus. The risk of transmission is less than 2%; in contrast, if the gestational parent does not take antiretroviral drugs, the risk is elevated to 25% (CDC, 2016b). However, the long-term risks of prenatal exposure to the medication are not known. It is recommended that people with HIV deliver the child by c-section and that after birth they avoid breastfeeding.
German Measles (or Rubella)
Rubella, also called German measles, is an infection that causes mild flu-like symptoms and a rash on the skin (March of Dimes, 2012a). Rubella in the gestational parent has been associated with various birth defects. If the gestational parent contracts the disease during the first three months of pregnancy, damage can occur in the eyes, ears, heart, or brain of the unborn child. If the pregnant person has German measles before the 11th week of prenatal development, deafness is almost certain and brain damage can also result. People in the United States are much less likely to be afflicted with rubella because most receive childhood vaccinations that protect them from the disease (March of Dimes, 2012a).
4.3 Maternal Factors
Gestational Parents Over Age 35
Most people over 35 who become pregnant are in good health and have healthy pregnancies. However, according to the March of Dimes (2016d), people over age 35 have an increased risk of:
- Fertility problems
- High blood pressure
- Diabetes
- Miscarriages
- Placenta Previa
- Cesarean section
- Premature birth
- Stillbirth
- A baby with a genetic disorder or other birth defects
Because a gestational parent is born with all their eggs, environmental teratogens can affect the quality of the eggs as they get older. Also, their reproductive system ages which can adversely affect the pregnancy. Some people over 35 choose special prenatal screening tests, such as a maternal blood screening, to determine if there are any health risks for the baby.
Although there are medical concerns associated with having a child later in life, there are also many positive consequences to being a more mature parent. Older parents are more confident, less stressed, and typically married, which can provide family stability. Their children perform better on math and reading tests, and they are less prone to injuries or emotional troubles (Albert, 2013). People who choose to wait are often well-educated and lead healthy lives. According to Gregory (2007), older women are more stable, demonstrate a stronger family focus, possess greater self-confidence, and have more money. Having a child later in one’s career equals overall higher wages. For every year gestational parents delays becoming a parent, they make 9% more in lifetime earnings. Lastly, gestational parents who delay having children live longer. Sun et al. (2015) found that women who had their last child after the age of 33 doubled their chances of living to age 95 or older than women who had their last child before their 30th birthday. A gestational parent’s natural ability to have a child at a later age indicates that their reproductive system is aging slowly, and consequently so is the rest of their body.
 Teenage Pregnancy
Teenage Pregnancy
A teenage gestational parent is at a greater risk for complications during pregnancy, including anemia and high blood pressure. These risks are even greater for those under age 15. Infants born to teenage gestational parents have a higher risk of being born prematurely and having low birth weight or other serious health problems. Premature and low birthweight babies may have organs that are not fully developed which can result in breathing problems, bleeding in the brain, vision loss, and serious intestinal problems. Very low birthweight babies (less than 3 1/3 pounds) are more than 100 times as likely to die, and moderately low birthweight babies (between 3 1/3 and 5 ½ pounds) are more than 5 times as likely to die in their first year, than normal weight babies (March of Dimes, 2012c). Again, the risk is highest for babies of gestational parents under age 15. A primary reason for these health issues is that teenagers are the least likely of all age groups to get early and regular prenatal care. Additionally, they may engage in risky behaviors during pregnancy, including eating unhealthy food, smoking, drinking alcohol, and taking drugs. Additional concerns for teenagers are repeat births. About 25% of teen gestational parents under age 18 have a second baby within 2 years after the first baby’s birth.
Gestational Diabetes
Seven percent of pregnant people develop gestational diabetes (March of Dimes, 2015b). Diabetes is a condition where the body has too much glucose in the bloodstream. Most pregnant people have their glucose level tested at 24 to 28 weeks of pregnancy. Gestational diabetes usually goes away after the gestational parent gives birth, but it might indicate a risk for developing diabetes later in life. If untreated, gestational diabetes can cause premature birth, stillbirth, infant breathing problems at birth, jaundice, or low blood sugar. Babies born to mothers with gestational diabetes can also be considerably heavier (more than 9 pounds) making the labor and birth process more difficult. For expectant mothers, untreated gestational diabetes can cause preeclampsia (high blood pressure and signs that the liver and kidneys may not be working properly) discussed later in the chapter. Risk factors for gestational diabetes include age (being over age 25), being overweight or gaining too much weight during pregnancy, a family history of diabetes, having had gestational diabetes with a prior pregnancy, and race and ethnicity (mothers who are African American, Native American, Hispanic, Asian, or Pacific Islander have a higher risk). Eating healthy food and maintaining a healthy weight during pregnancy can reduce the chance of gestational diabetes. People who already have diabetes and become pregnant need to attend all their prenatal care visits and follow the same advice as those for people with gestational diabetes as the risk of preeclampsia, premature birth, birth defects, and stillbirth is the same.
High Blood Pressure (Hypertension)
Hypertension is a condition in which the pressure against the wall of the arteries becomes too high. There are two types of high blood pressure during pregnancy, gestational and chronic. Gestational hypertension only occurs during pregnancy and goes away after birth. Chronic high blood pressure refers to people who already had hypertension before the pregnancy or to those who developed it during pregnancy, and it continued after birth. According to the March of Dimes (2015c) about 8 in every 100 pregnant people have high blood pressure. High blood pressure during pregnancy can cause premature birth and low birth weight (under five and a half pounds), placental abruption, and mothers can develop preeclampsia.
Rh Disease
Rh is a protein found in the blood. Most people are Rh-positive, meaning they have this protein. Some people are Rh-negative, meaning this protein is absent. Gestational parents who are Rh-negative are at risk of having a baby with a form of anemia called Rh disease (March of Dimes, 2009). A father who is Rh-positive and gestational parent who is Rh-negative can conceive a baby who is Rh-positive. Some of the fetus’s blood cells may get into the gestational parent’s bloodstream and their immune system is unable to recognize the Rh factor. The immune system starts to produce antibodies to fight off what it thinks is a foreign invader. Once the pregnant person’s body produces immunity, the antibodies can cross the placenta and start to destroy the red blood cells of the developing fetus. As this process takes time, often the first Rh-positive baby is not harmed, but because the pregnant person’s body continues to produce antibodies to the Rh factor across their lifetime, subsequent pregnancies can pose a greater risk for a Rh-positive baby. In newborns, Rh disease can lead to jaundice, anemia, heart failure, brain damage, and death.
Weight Gain During Pregnancy
According to March of Dimes (2016f) during pregnancy, most people need only an additional 300 calories per day to aid in the growth of the fetus. Gaining too little or too much weight during pregnancy can be harmful. People who gain too little may have a baby who is at a low-birth weight, while those who gain too much are likely to have a premature or large baby. There is also a greater risk of the gestational parent developing preeclampsia and diabetes, which can cause further problems during the pregnancy. Table 5.1 shows the healthy weight gain during pregnancy. Putting on the weight slowly is best. Gestational parents who are concerned about their weight gain should talk to their healthcare provider.
Table on Weight Gain During Pregnancy
| If you were a healthy weight before pregnancy | If you were underweight before pregnancy | If you were overweight before pregnancy | If you were obese before pregnancy |
|---|---|---|---|
|
|
|
|
|
*Note - Gestational parents of multiples need to gain more in each of the categories listed above in the table.
Stress
It is common to feel stressed during pregnancy, but high levels of stress can cause complications including having a premature or low-birthweight baby. Babies born early or too small are at an increased risk for health problems. Stress-related hormones may cause these complications by affecting a gestational parent’s immune system resulting in an infection and premature birth. Additionally, some people deal with stress by smoking, drinking alcohol, or taking drugs, which can lead to problems in the pregnancy. High levels of stress in pregnancy have also been correlated with problems in the baby’s brain development and immune system functioning, as well as childhood problems such as trouble paying attention and anxiety (March of Dimes, 2012b).
Depression
Depression is a significant medical condition in which feelings of sadness, worthlessness, guilt, and fatigue interfere with one’s daily functioning. Depression can occur before, during, or after pregnancy, and 1 in 7 pregnant people are treated for depression sometime between the year before pregnancy and the year after pregnancy (March of Dimes, 2015a). People who have experienced depression previously are more likely to have depression while pregnant. Consequences of depression include the baby being born prematurely, having a low birth weight, being more irritable, less active, less attentive, and having fewer facial expressions. About 13% of pregnant people take an antidepressant during pregnancy. Pregnant people taking antidepressants must discuss the medication with a health care provider as some medications can cause harm to the developing organism. Birth defects are about 2 to 3 times more likely in people who are prescribed certain Selective Serotonin Reuptake Inhibitors (SSRIs) for their depression.
Paternal Impact
The age of fathers at the time of conception is also an important factor in health risks for children. According to Nippoldt (2015) offspring of men over 40 face an increased risk of miscarriage, autism, birth defects, achondroplasia (bone growth disorder), and schizophrenia. These increased health risks are thought to be due to chromosomal aberrations and mutations that accumulate during the maturation of sperm cells in older men (Bray et al., 2006). However, like older women, the overall risks are small.
In addition, men are more likely than women to work in occupations where hazardous chemicals, many of which have teratogenic effects or may cause genetic mutations, are used (Cordier, 2008). These may include petrochemicals, lead, and pesticides that can cause abnormal sperm and lead to miscarriages or diseases. Men are also more likely to be a source of secondhand smoke for their developing offspring. As noted earlier, smoking by either the mother or around the gestational parent can impede prenatal development.
Complications of Pregnancy
There are several common side effects of pregnancy. Not everyone experiences all of these nor do gestational parents experience them to the same degree. And although they are considered “minor” these problems are potentially very uncomfortable. These side effects include nausea (particularly during the first 3-4 months of pregnancy because of higher levels of estrogen in the system), heartburn, gas, hemorrhoids, backache, leg cramps, insomnia, constipation, shortness of breath or varicose veins (as a result of carrying a heavy load on the abdomen). What is the current cure? Delivery!
Link to Learning – Could morning sickness be cured?
According to multiple news outlets, including ABC News and CNN, a research article published in the academic journal Nature has discovered that “some pregnant people are particularly sensitive to a hormone called GDF15” (Christensen, 2023, para. 3). Normally, the hormone is produced in low levels, but when a person becomes pregnant, they can receive a large dose of from the growing fetus. Studies done with cancer patients have confirmed that a large of the hormone can cause nausea and vomiting. This new study confirms a large body of research also conducted in lab tests and tests with mice (Christensen, 2023).
Why are these findings important?
Morning sickness can lead to severe dehydration and weight loss. In addition, it can have negative effects on the baby “including causing premature, neurodevelopmental disorders or even miscarriage” (Christensen, 2023, para. 8). While there are some medicinal remedies that can be taken to fight morning sickness, not all methods are effective. Thus, discovering the underlying cause of the ailment gets researchers much closer to finding a more effective solution for both cancer patients and pregnant persons.
4.4 Major Complications of Pregnancy
The following are some serious complications of pregnancy that can pose health risks to the gestational parent and child and that often require special care.
- Gestational diabetes is when a gestational parent without diabetes develops high blood sugar levels during pregnancy.
- Hyperemesis gravidarum is the presence of severe and persistent vomiting, causing dehydration and weight loss. It is more severe than the more common morning sickness.
- Preeclampsia is gestational hypertension. Severe preeclampsia involves blood pressure over 160/110 with additional signs. Eclampsia is seizures in a pre-eclamptic patient.
- Deep vein thrombosis is the formation of a blood clot in a deep vein, most commonly in the legs.
- A pregnant person is more susceptible to infections. This increased risk is caused by an increased immune tolerance in pregnancy to prevent an immune reaction against the fetus.
- Peripartum cardiomyopathy is a decrease in heart function that occurs in the last month of pregnancy, or up to six months post-pregnancy.
Maternal Mortality
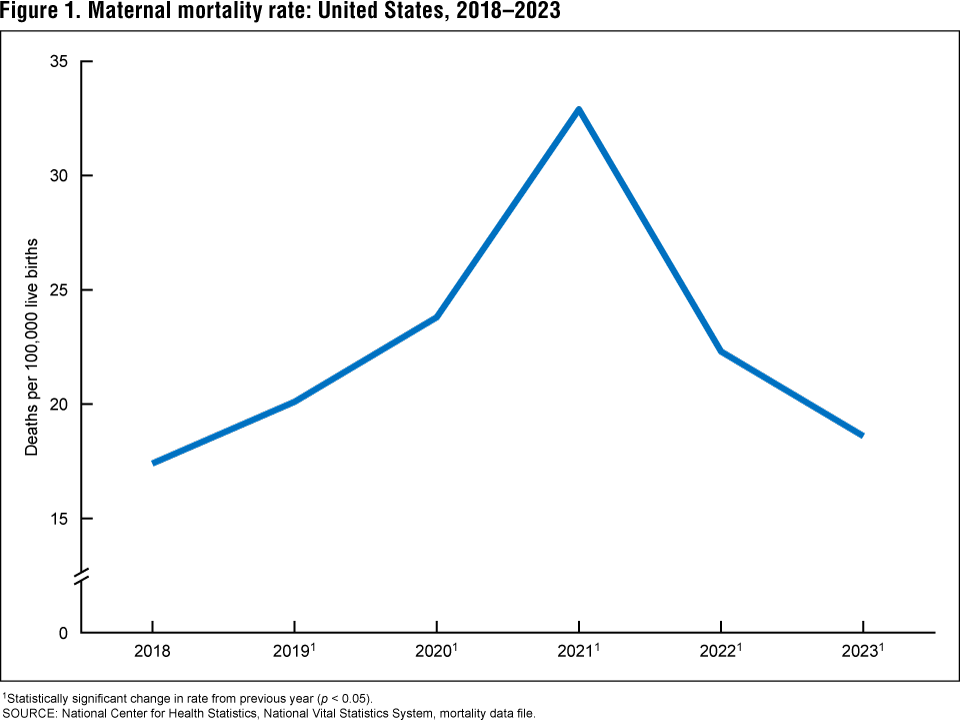
Maternal mortality over the past few decades has been unacceptably high in the United States, however, the recent data collected by the U.S. National Center for Health Statistics shows a significant decrease in 2023 in the maternal mortality rate (MMR). According to the NCHS (2025), the overall decrease in the maternal mortality rate in the United States from 22.3 deaths per 100,000 live births in 2022 to 18.6 in 2023 is a positive development, indicating potential improvements in maternal healthcare or reporting (review figure 1 below).
This reduction was statistically significant for White non-Hispanic and Hispanic women, suggesting that interventions or systemic changes may be having a more immediate and measurable impact on these demographic groups. While this decline is encouraging, an increase for Black non-Hispanic women and decrease for Asian non-Hispanic women highlights the persistent racial disparities in maternal health outcomes.
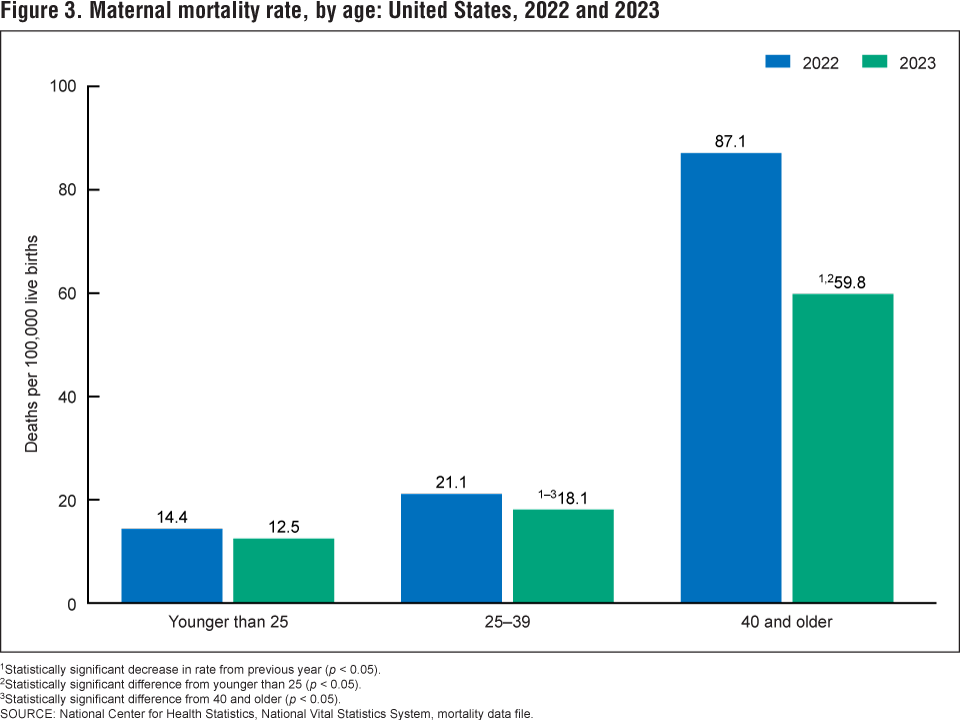
A critical implication of this data is the stark and continuing racial inequity in maternal mortality. Black women faced a maternal mortality rate of 50.3 deaths per 100,000 live births in 2023, which is significantly higher—nearly three to five times greater—than the rates for White (14.5), Hispanic (12.4), and Asian (10.7) women (Hoyert, 2025). This disparity underscores the need for targeted public health initiatives, policy changes, and healthcare interventions that address the social, economic, and systemic factors contributing to poorer maternal health outcomes for Black women. Without focused efforts, these inequities are likely to persist, exacerbating existing health disparities (Review figure 2 below). 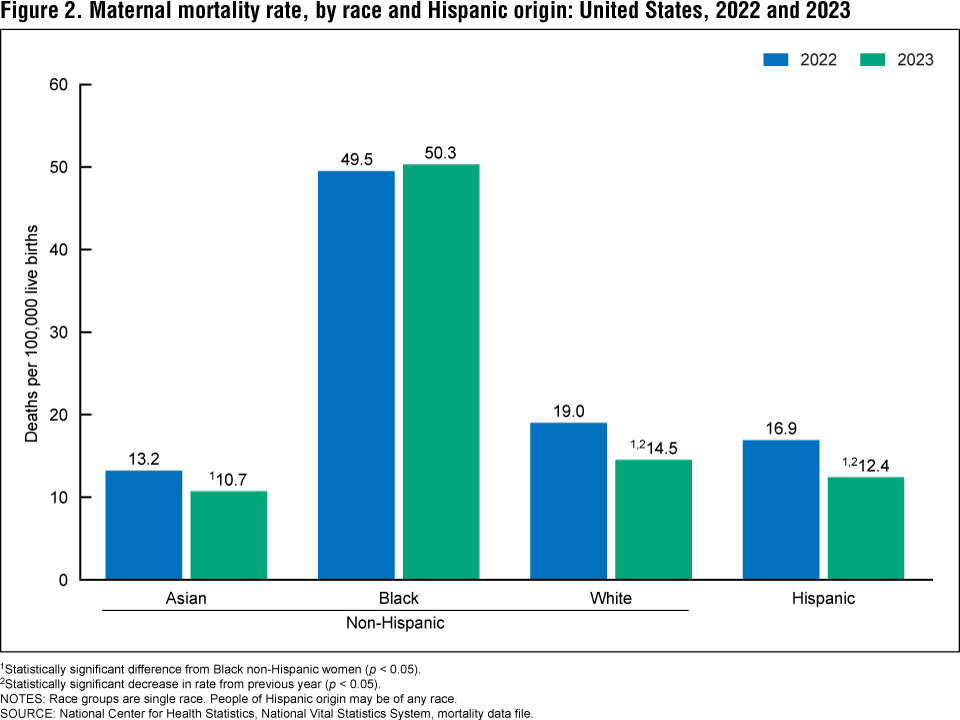 Furthermore, the data reveals significant age-related implications, with older women facing substantially higher risks. The maternal mortality rate for women aged 40 and older was 59.8 deaths per 100,000 live births, nearly five times higher than for those younger than 25. While rates decreased significantly for women ages 25-39 and 40 and older between 2022 and 2023, the inherent risk associated with advanced maternal age remains a critical factor (Hoyert, 2025). This suggests a need for increased vigilance, specialized care, and comprehensive risk assessments for older pregnant individuals to decrease potential complications and improve outcomes.
Furthermore, the data reveals significant age-related implications, with older women facing substantially higher risks. The maternal mortality rate for women aged 40 and older was 59.8 deaths per 100,000 live births, nearly five times higher than for those younger than 25. While rates decreased significantly for women ages 25-39 and 40 and older between 2022 and 2023, the inherent risk associated with advanced maternal age remains a critical factor (Hoyert, 2025). This suggests a need for increased vigilance, specialized care, and comprehensive risk assessments for older pregnant individuals to decrease potential complications and improve outcomes.
 Miscarriage
Miscarriage
Spontaneous abortion is experienced in an estimated 20-40 percent of undiagnosed pregnancies and in another 10 percent of diagnosed pregnancies. Usually, the body aborts due to chromosomal abnormalities and this typically happens before the 12th week of pregnancy. Cramping and bleeding result and normal periods return after several months. Some gestational parents are more likely to have repeated miscarriages due to chromosomal, amniotic, or hormonal problems; but miscarriage can also be a result of defective sperm (Carroll et al., 2003).
References
Albert, E. (2013). Many more women delay childbirth into 40s due to career constraints. Milwaukee Journal Sentinel. http://www.jsonline.com/news/health/many-more-women-delay-childbirth-into-40s-due-to-career-constraints-b9971144z1-220272671.html
Betts, J. G., DeSaix, P., Johnson, E., Johnson, J. E., Korol, O., Kruse, D. H., Poe, B., Wise, J. A., & Young, K. A. (2019). Anatomy and physiology (OpenStax). Rice University.
Berger, K. S. (2005). The developing person through the life span (6 ed.). Worth.
Bray, I., Gunnell, D., & Smith, G. D. (2006). Advanced paternal age: How old is too old? Journal of Epidemiology & Community Health, 60(10), 851-853. doi: 10.1136/jech.2005.045179
Carrell, D. T., Wilcox, A. L., Lowry, L., Peterson, C. M., Jones, K. P., & Erikson, L. (2003). Elevated sperm chromosome aneuploidy and apoptosis in patients with unexplained recurrent pregnancy loss. Obstetrics and Gynecology, 101(6), 1229-1235.
Centers for Disease Control and Prevention. (2005). Surgeon’s general’s advisory on alcohol use during pregnancy. https://www.cdc.gov/ncbddd/fasd/documents/surgeongenbookmark.pdf
Centers for Disease Control and Prevention. (2016a). Fetal alcohol spectrum disorders. http://www.cdc.gov/ncbddd/fasd
Centers for Disease Control and Prevention. (2016b). HIV/AIDS prevention. http://www.cdc.gov/hiv/basics/prevention.html
Centers for Disease Control and Prevention. (2016c). HIV transmission. http://www.cdc.gov/hiv/basics/transmission.html
Centers for Disease Control and Prevention. (2016d). STDs during pregnancy. http://www.cdc.gov/std/pregnancy/stdfact-pregnancy.htm
Centers for Disease Control and Prevention. (2015d). Smoking, pregnancy, and babies. http://www.cdc.gov/tobacco/campaign/tips/diseases/pregnancy.html
Christensen, J. (2003, December 15). Scientists may have found the cause of morning sickness and see hope for treatment. CNN. https://www.cnn.com/2023/12/15/health/cause-of-morning-sickness-wellness/index.html
Cordier, S. (2008). Evidence for a role of paternal exposure in developmental toxicity. Basic and Clinical Pharmacology and Toxicology, 102, 176-181.
Gregory, E. (2007). Ready: Why women are embracing the new later motherhood. Basic Books.
Grossman, D., & Slutsky, D. (2017). The effect of an increase in lead in the water system on fertility and birth outcomes: The case of Flint, Michigan. Economics Faculty Working Papers Series. http://www2.ku.edu/~kuwpaper/2017Papers/201703.pdf
Hall, D. (2004). Meiotic drive and sex chromosome cycling. Evolution, 58(5), 925-931.
Hoyert, D.L. (2025). Maternal mortality rates in the United States, 2023. (Health E-Stats) National Center for Health Statistics. https://dx.doi.org/10.15620/cdc/174577
Maier, S.E., & West, J.R. (2001). Drinking patterns and alcohol-related birth defects. Alcohol Research & Health, 25(3), 168-174.
March of Dimes. (2009). Rh disease. http://www.marchofdimes.org/complications/rh-disease.aspx
March of Dimes. (2012a). Rubella and your baby. http://www.marchofdimes.org/baby/rubella-and-your-baby.aspx
March of Dimes. (2012b). Stress and pregnancy. http://www.marchofdimes.org/pregnancy/stress-and-pregnancy.aspx
March of Dimes. (2012c). Teenage pregnancy. http://www.marchofdimes.org/materials/teenage-pregnancy.pdf
March of Dimes. (2012d). Toxoplasmosis. http://www.marchofdimes.org/complications/toxoplasmosis.aspx
March of Dimes. (2013). Sexually transmitted diseases. http://www.marchofdimes.org/complications/sexually-transmitted-diseases.aspx
March of Dimes. (2014). Pesticides and pregnancy. http://www.marchofdimes.org/pregnancy/pesticides-and-pregnancy.aspx
March of Dimes. (2015a). Depression during pregnancy. http://www.marchofdimes.org/complications/depression-during-pregnancy.aspx
March of Dimes. (2015b). Gestational diabetes. http://www.marchofdimes.org/complications/gestational-diabetes.aspx
March of Dimes. (2015c). High blood pressure during pregnancy. http://www.marchofdimes.org/complications/high-blood-pressure-during-pregnancy.aspx
March of Dimes. (2015d). Neonatal abstinence syndrome. http://www.marchofdimes.org/complications/neonatal-abstinence-syndrome-(nas).aspx
March of Dimes. (2016a). Fetal alcohol spectrum disorders. http://www.marchofdimes.org/complications/fetal-alcohol-spectrum-disorders.aspx
March of Dimes. (2016b). Identifying the causes of birth defects. http://www.marchofdimes.org/research/identifying-the-causes-of-birth-defects.aspx
March of Dimes. (2016c). Marijuana and pregnancy. http://www.marchofdimes.org/pregnancy/marijuana.aspx
March of Dimes. (2016d). Pregnancy after age 35. http://www.marchofdimes.org/pregnancy-after-age-35.aspx
March of Dimes. (2016e). Prescription medicine during pregnancy. http://www.marchofdimes.org/pregnancy/prescription-medicine-during-pregnancy.aspx
March of Dimes. (2016f). Weight gain during pregnancy. http://www.marchofdimes.org/pregnancy/weight-gain-during-pregnancy.aspx
World Health Organization. (n.d.). Maternal mortality. https://www.who.int/news-room/fact-sheets/detail/maternal-mortality.
Morgan, M.A., Goldenberg, R.L., & Schulkin, J. (2008). Obstetrician-gynecologists’ practices regarding preterm birth at the limit of viability. The Journal of Maternal-Fetal and Neonatal Medicine, 21, 115-121.
Nippoldt, T.B. (2015). How does paternal age affect a baby’s health? Mayo Clinic. http://www.mayoclinic.org/healthy-lifestyle/getting-pregnant/expert-answers/paternal-age/faq– 20057873
Poduri, A., & Volpe, J. (2018). Volpe’s neurology of the newborn (6th edition). Elsevier.
Rehan, V. K., Sakurai, J. S., & Torday, J. S. (2011). Thirdhand smoke: A new dimension to the effects of cigarette smoke in the developing lung. American Journal of Physiology: Lung Cellular and Molecular Physiology, 301(1), L1-8.
Royal College of Obstetricians and Gynecologists. (1997). Fetal awareness: Review of research and Recommendations. https://www.rcog.org.uk/en/guidelines-research-services/guidelines/fetal-awareness—review-of-research-and-recommendations-for-practice/
Someji, S., & Beltrán-Sánchez, H. (2019). Association of maternal cigarette smoking and smoking cessation with preterm birth. JAMA Network Open, 2(4), doi:10.1001/jamanet\workopen.2514
Stiles, J. & Jernigan, T. L. (2010). The basics of brain development. Neuropsychology Review, 20(4), 327-348. doi: 10.1007/s11065-010-9148-4
Streissguth, A.P., Barr, H.M., Kogan, J. & Bookstein, F. L. (1996). Understanding the occurrence of secondary disabilities in clients with Fetal Alcohol Syndrome (FAS) and Fetal Alcohol Effects (FAE). Final Report to the Centers for Disease Control and Prevention (CDC), August. Seattle: University of Washington, Fetal Alcohol & Drug Unit, Tech. Rep. No. 96-06.
Sun, F., Sebastiani, P., Schupf, N., Bae, H., Andersen, S. L., McIntosh, A., Abel, H., Elo, I., & Perls, T. (2015). Extended maternal age at birth of last child and women’s longevity in the Long Life Family Study. Menopause: The Journal of the North American Menopause Society, 22(1), 26-31.
Tong, V. T., Dietz, P.M., Morrow, B., D’Angelo, D.V., Farr, S.L., Rockhill, K.M., & England, L.J. (2013). Trends in smoking before, during, and after pregnancy — Pregnancy Risk Assessment Monitoring System, United States, 40 Sites, 2000–2010. Surveillance Summaries, 62(SS06), 1-19. http://www.cdc.gov/mmwr/preview/mmwrhtml/ss6206a1.htm
United States National Library of Medicine. (2015). Fetal development. https://www.nlm.nih.gov/medlineplus/ency/article/002398.htm
Wisconsin Department of Health Services (2025, April 17). New data show congenital syphilis increasing in Wisconsin while other Sexually Transmitted Infections (STIs) decrease [Press Release]. https://www.dhs.wisconsin.gov/news/releases/041725.htm#:~:text=Syphilis%20cases%20overall%20have%20continued,to%20a%20baby%20during%20pregnancy.
Youngentob, S. L., Molina, J. C., Spear, N. E., & Youngentob, L. M. (2007). The effect of gestational ethanol exposure on voluntary ethanol intake in early postnatal and adult rats. Behavioral Neuroscience, 121(6), 1306-1315. doi.org/10.1037/0735-7044.121.6.1306
Media Attributions
- 6867005898_94d03edea7_q © Yorgos Nikas is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- Germinal Period © Unknown Name is licensed under a CC BY-SA (Attribution ShareAlike) license
- Embyonic Period © Lunar Caustic is licensed under a CC BY-SA (Attribution ShareAlike) license
- Prenatal stages is licensed under a CC BY-SA (Attribution ShareAlike) license
- FAS © Teresa Kellerman is licensed under a CC BY-SA (Attribution ShareAlike) license
- Cat in a litter box © Tom Thai is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}
{kind=link}
{kind=link}