Section 5: Infancy and Toddlerhood
5.1 Physical Development in Infancy and Toddlerhood
What’s physical development like in the first two years?

We’ll begin this section by reviewing the physical development that occurs during infancy, a period that starts at birth and continues until the second birthday. We’ll see how this time involves rapid growth, not only in observable changes like height and weight but also in brain development.
Next, we will explore reflexes. At birth, infants are equipped with a number of reflexes, which are involuntary movements in response to stimulation. We will explore these innate reflexes and then consider how these involuntary reflexes eventually modify through experiences to become voluntary movements and the basis for motor development as skills emerge that allow an infant to grasp food, roll over, and take the first step.
Third, we will explore the baby’s senses. Every sense functions at birth—newborns use all of their senses to attend to everything and every person. We will explore how infants’ senses develop, how sensory systems like hearing and vision operate, and how infants take in information through their senses and transform it into meaningful information.
Finally, since growth during infancy is so rapid and the consequence of neglect can be severe, we will consider some of the influences on early physical growth, particularly the importance of nutrition.
Learning Objectives
- Summarize overall physical growth patterns during infancy
- Describe the growth of the brain during infancy
- Explain gross and fine motor skills in infants
- Explain newborn perceptual abilities
- Describe sleep concerns for infants
- Explain how vaccines work and their impact on public health
Physical Growth and Brain Development in Infancy
Overall Physical Growth
By the time an infant is 4 months old, it usually doubles in weight and has tripled its birth weight by one year. By age 2, the weight has quadrupled. The average length at 12 months (one year old) typically ranges from 28.5-30.5 inches. The average length at 24 months (two years old) is around 33.2-35.4 inches (CDC, 2010).

Monitoring Physical Growth
As mentioned earlier, growth is so rapid in infancy that the consequences of neglect can be severe. For this reason, gains are closely monitored. At each well-baby check-up, a baby’s growth is compared to that baby’s previous numbers. Often, measurements are expressed as a percentile from 0 to 100, which compares each baby to other babies the same age. For example, weight at the 40th percentile means that 40 percent of all babies weigh less, and 60 percent weigh more. For any baby, pediatricians and parents can be alerted early just by watching percentile changes. If an average baby moves from the 50th percentile to the 20th, this could be a sign of failure to thrive, which could be caused by various medical conditions or factors in the child’s environment. The earlier the concern is detected, the earlier intervention and support can be provided for the infant and caregiver.
Body Proportions
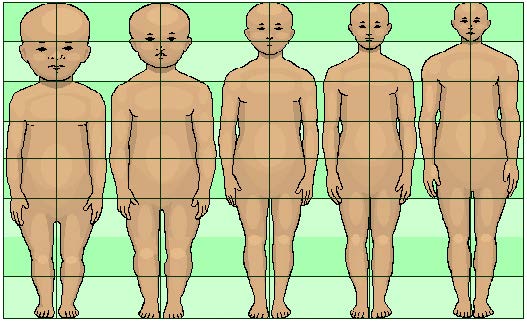
Another dramatic physical change that takes place in the first several years of life is a change in body proportions. The head initially makes up about 50 percent of a person’s entire length when developing in the womb. At birth, the head makes up about 25 percent of a person’s length (just imagine how big your head would be if the proportions remained the same throughout your life!). In adulthood, the head comprises about 15 percent of a person’s length. Imagine how difficult it must be to raise one’s head during the first year of life! And indeed, if you have ever seen a 2- to 4-month-old infant lying on their stomach trying to raise their head, you know how much of a challenge this is (Figure 2).
The Brain in the First Two Years
Some of the most dramatic physical change that occurs during this period is in the brain. At birth, the brain is about 25 percent of its adult weight, and this is not true for any other part of the body. By age 2, it is at 75 percent of its adult weight, at 95 percent by age 6, and at 100 percent by age 7 years. We are born with most of the brain cells that we will ever have; that is, about 85 billion neurons whose function is to store and transmit information (Huttenlocher & Dabholkar, 1997).

Organization of high-level visual cortex in human infants”. Image retrieved from https://www.quantamagazine.org/infant-brains-reveal-how-the-mind-gets-built-20170110/.
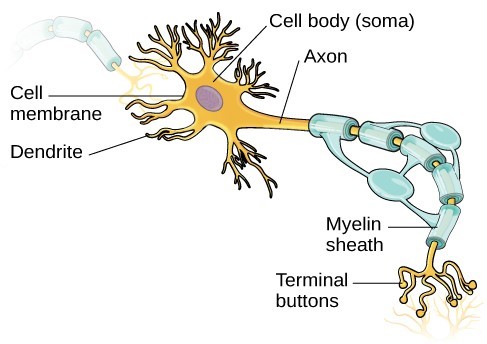
Communication within the central nervous system (CNS), which consists of the brain and spinal cord, begins with nerve cells called neurons. Neurons connect to other neurons via networks of nerve fibers called axons and dendrites. Each neuron typically has a single axon and numerous dendrites, which are spread out like branches of a tree (some will say it looks like a hand with fingers). The axon of each neuron reaches toward the dendrites of other neurons at intersections called synapses, which are critical communication links within the brain. Axons and dendrites do not touch. Instead, electrical impulses in the axons cause the release of chemicals called neurotransmitters, which carry information from the axon of the sending neuron to the dendrites of the receiving neuron.
While most of the brain’s neurons are present at birth, they are not fully mature. During the next several years dendrites, or branching extensions that collect information from other neurons, will undergo a period of exuberance. Because of this proliferation of dendrites, by age two, a single neuron might have thousands of dendrites. Synaptogenesis, or the formation of connections between neurons, continues from the prenatal period, forming thousands of new connections during infancy and toddlerhood. This period of rapid neural growth is referred to as synaptic blooming (see Figure 4).
The blooming period of neural growth is followed by a period of synaptic pruning, where neural connections are reduced, thereby making those that are used much stronger. It is thought that pruning causes the brain to function more efficiently, allowing for mastery of more complex skills (Kolb, B. & Whishaw, 2011). Experience will shape which of these connections are maintained and which of these are lost. Ultimately, about 40 percent of these connections will be lost (Webb et al., 2001). Blooming occurs during the first few years of life, and pruning continues through childhood and into adolescence in various areas of the brain.
Another major change occurring in the central nervous system is the development of myelin, a coating of fatty tissues around the axon of the neuron (Carlson, 2014). Myelin helps insulate the nerve cell and speed the rate of transmission of impulses from one cell to another. This enhances the building of neural pathways and improves coordination, movement control, and thought processes. The development of myelin continues into adolescence but is most dramatic during the first several years of life.
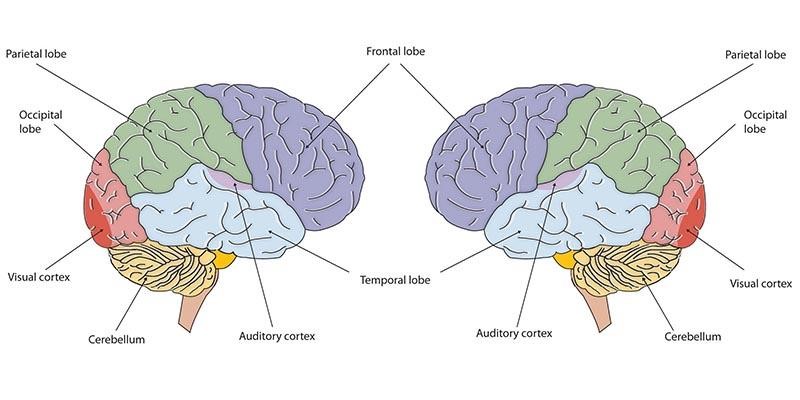
Most of the neural activity occurs in the cortex or the thin outer covering of the brain involved in voluntary activity and thinking. The cortex has two hemispheres, and each hemisphere is divided into four lobes, each separated by folds known as fissures. If we look at the cortex starting at the front of the brain and moving over the top (see Figure 5), we see first the frontal lobe (behind the forehead), which is responsible primarily for thinking, planning, memory, and judgment. Following the frontal lobe is the parietal lobe, which extends from the middle to the back of the skull and which is responsible primarily for processing information about touch. Next is the occipital lobe, at the very back of the skull, which processes visual information. Finally, in front of the occipital lobe, between the ears, is the temporal lobe, which is responsible for hearing and language.
Although the brain grows rapidly during infancy, specific brain regions do not mature at the same rate. Primary motor areas develop earlier than primary sensory areas, and the prefrontal cortex, which is located behind the forehead, is the least developed. Experience will shape which of these connections are maintained and which of these are lost. Ultimately, about 40 percent of these connections will be lost (Webb et al., 2001). As the prefrontal cortex matures, the child is increasingly able to regulate or control emotions, plan activities, strategize, and have better judgment. Of course, this is not fully accomplished in infancy and toddlerhood but continues throughout childhood and adolescence.
Lateralization is the process in which different functions become localized primarily on one side of the brain. For example, in most adults, the left hemisphere is more active than the right during language production, while the reverse pattern is observed during tasks involving visuospatial abilities (Springer & Deutsch, 1993). This process develops over time. However, structural asymmetries between the hemispheres have been reported even in fetuses (Chi, Dooling, & Gilles, 1977; Kasprian, et al., 2011) and infants (Dubois, J., et al., 2009).
Lastly, neuroplasticity refers to the brain’s ability to change, both physically and chemically, to enhance its adaptability to environmental change and compensate for injury. Both environmental experiences, such as stimulation, and events within a person’s body, such as hormones and genes, affect the brain’s plasticity. So, too, does age. Adult brains demonstrate neuroplasticity, but they are influenced more slowly and less extensively than those of youth (Kolb & Gibb, 2011).
Motor and Sensory Development
From Reflexes to Voluntary Movements
Every basic motor skill (any movement ability) develops over the first two years of life. The sequence of motor skills first begins with reflexes. Infants are equipped with a number of reflexes or involuntary movements in response to stimulation, and some are necessary for survival. These include the breathing reflex, or the need to maintain an oxygen supply (this includes hiccups, sneezing, and thrashing reflexes), reflexes that maintain body temperature (crying, shivering, tucking the legs close, and pushing away blankets), the sucking reflex, or automatically sucking on objects that touch their lips, and the rooting reflex, which involves turning toward any object that touches the cheek (which manages feeding, including the search for a nipple).
Other reflexes are not necessary for survival but signify the state of brain and body functions. Some of these include the Babinski reflex (toes fan upward when feet are stroked), the stepping reflex (babies move their legs as if to walk when feet touch a flat surface), the palmar grasp (the infant will tightly grasp any object placed in its palm), and the Moro reflex (babies will fling arms out and then bring to the chest if they hear a loud noise). These movements occur automatically and are signals that the infant is functioning well neurologically. Within the first several weeks of life, these reflexes are replaced with voluntary movements or motor skills.
Some of the more common reflexes, such as the sucking reflex (infants suck on objects that touch their lips automatically) and the rooting reflex, are essential to feeding. The grasping and stepping reflexes are eventually replaced by more voluntary behaviors. Within the first few months of life, these reflexes disappear, while other reflexes, such as the eye-blink, swallowing, sneezing, gagging, and withdrawal reflexes, stay with us as they continue to serve essential functions. Reflexes offer insight into the maturation and health of the nervous system. Reflexes that persist too long may impede healthy development (Berne, 2006; Bloem, M. 2007). In preterm infants and those with neurological impairments, some of these reflexes may be absent at birth. Once present, they may persist longer than in a neurologically healthy infant (El-Dib, et al., 2012).
Motor development
Motor development occurs in an orderly sequence as infants move from reflexive reactions (e.g., sucking and rooting) to more advanced motor functioning. This development proceeds in a cephalocaudal (from head-down) and proximodistal (from center-out) direction. Gross Motor Skills refer to our ability to move our bodies and manipulate objects. Fine motor skills focus on the muscles in our fingers, toes, and eyes and enable coordination of small actions (e.g., grasping a toy, writing with a pencil, and using a spoon).
Newborns cannot grasp objects voluntarily but do wave their arms toward objects of interest. At about 4 months of age, the infant is able to reach for an object, first with both arms and, within a few weeks, with only one arm. At this age, grasping an object involves the use of the fingers and palm, but no thumbs. This is known as the palmar grasp. The use of the thumb comes at about 9 months of age when the infant is able to grasp an object using the forefinger and thumb. Now, the infant uses a pincer grasp, and this ability greatly enhances the ability to control and manipulate an object and infants take great delight in this newfound ability. They may spend hours picking up small objects from the floor and placing them in containers. By 9 months, an infant can also watch a moving object, reach for it as it approaches, and grab it.
As motor skills develop, there are certain developmental milestones that young children should achieve. For each milestone, there is an average age, as well as a range of ages in which the milestone should be reached. An example of a developmental milestone is a baby holding up its head. Babies, on average, are able to hold up their head at 6 weeks old, and 90% of babies achieve this between 3 weeks and 4 months old. If a baby is not holding up his head by 4 months old, he is showing a delay.
On average, most babies sit alone at 7 months old. Sitting involves both coordination and muscle strength, and 90% of babies achieve this milestone between 5 and 9 months old (CDC, 2018). If the child is displaying delays on several milestones, that is a reason for concern, and the parent or caregiver should discuss this with the child’s pediatrician. Some developmental delays can be identified and addressed through early intervention.
Link to Learning
It is important to understand that there is a range of normal for reaching developmental milestones. It should not be a competition between parents whose child reached which milestones first. Each child will develop at their own pace based on many different factors. However, if a delay is diagnosed there are early invention services that are available in most states. Review the services that are available in California.
Gross Motor Skills

Gross motor skills focus on large muscle groups that control our head, torso, arms, and legs and involve larger movements (e.g., balancing, running, and jumping). These skills begin to develop first. Examples include moving to bring the chin up when lying on the stomach, moving the chest up, and rocking back and forth on hands and knees. But it also includes exploring an object with one’s feet as many babies do, as early as 8 weeks of age, if seated in a carrier or other device that frees the hips. This may be easier than reaching for an object with the hands, which requires much more practice (Berk, 2007). Sometimes, an infant will try to move toward an object while crawling and surprisingly move backward because of the greater amount of strength in the arms than in the legs!
Fine Motor Skills
Fine motor skills are more exact movements of the hands and fingers and include the ability to reach and grasp an object. These skills focus on the muscles in the fingers, toes, and eyes and enable coordination of small actions (e.g., grasping a toy, writing with a pencil, and using a spoon). Newborns cannot grasp objects voluntarily but do wave their arms toward objects of interest. At about 4 months of age, the infant is able to reach for an object, first with both arms and, within a few weeks, with only one arm. Grasping an object involves the use of the fingers and palm, but no thumbs. Stop reading for a moment and try to grasp an object using the fingers and the palm. How does that feel? How much control do you have over the object? If it is a pen or pencil, are you able to write with it? Can you draw a picture? The answer is probably not. Use of the thumb comes at about 9 months of age when the infant is able to grasp an object using the forefinger and thumb (the pincer grasp). This ability greatly enhances the ability to control and manipulate an object, and infants take great delight in this newfound ability. They may spend hours picking up small objects from the floor and placing them in containers. By 9 months, an infant can also watch a moving object, reach for it as it approaches, and grab it. This is quite a complicated set of actions if we remember how difficult this would have been just a few months earlier.
| Table 1. Timeline of Developmental Milestones. | |
| ~2 months |
|
| ~3 months |
|
| ~4-5 months |
|
| ~6 months |
|
| ~7-8 months |
|
| ~8-9 months |
|
| ~11-12 months |
|
| ~18 months |
|
| ~2 years |
|
| ~3 years |
|
| ~4 years |
|
| ~5 years |
|
Link to Learning
The Centers for Disease Control and Prevention (CDC) describes the developmental milestones for children from 2 months through 5 years old. After reviewing the information, take the CDC’s Developmental Milestones quiz to see how well you recall what you’ve learned. If you are a parent with concerns about your child’s development, contact your pediatrician.
Sensory Development
Throughout much of history, the newborn was considered a passive, disorganized being who possessed minimal abilities. However, current research techniques have demonstrated just how developed the newborn is with especially organized sensory and perceptual abilities.
As infants and children grow, their senses play a vital role in encouraging and stimulating the mind and in helping them observe their surroundings. Two terms are important to understand when learning about the senses. The first is sensation, or the interaction of information with the sensory receptors. The second is perception, or the process of interpreting what is sensed. It is possible for someone to sense something without perceiving it. Gradually, infants become more adept at perceiving with their senses, making them more aware of their environment and presenting more affordances or opportunities to interact with objects.
Vision
What can young infants see, hear, and smell? Newborn infants’ sensory abilities are significant, but their senses are not yet fully developed. Many of a newborn’s innate preferences facilitate interaction with caregivers and other humans.
The womb is a dark environment void of visual stimulation. Consequently, vision is the most poorly developed sense at birth. Newborns typically cannot see further than 8 to 16 inches away from their faces, have difficulty keeping a moving object within their gaze, and can detect contrast more than color differences. If you have ever seen a newborn struggle to see, you can appreciate the cognitive efforts being made to take in visual stimulation and build those neural pathways between the eye and the brain.
Although vision is their least developed sense, newborns already show a preference for faces. When you glance at a person, where do you look? Chances are you look into their eyes. If so, why? It is probably because there is more information there than in other parts of the face. Newborns do not scan objects this way; rather, they tend to look at the chin or another less detailed part of the face. However, by 2 or 3 months, they will seek more detail when visually exploring an object and begin showing preferences for unusual images over familiar ones, for patterns over solids, faces over patterns, and three-dimensional objects over flat images. Newborns have difficulty distinguishing between colors, but within a few months, are able to discriminate between colors as well as adults. Infants can also sense depth as binocular vision develops at about 2 months of age. By 6 months, the infant can perceive depth perception in pictures as well (Sen, Yonas, & Knill, 2001). Infants who have experience crawling and exploring will pay greater attention to visual cues of depth and modify their actions accordingly (Berk, 2007).
Hearing
The infant’s sense of hearing is very keen at birth. If you remember from an earlier module, this ability to hear is evidenced as soon as the 5th month of prenatal development. In fact, an infant can distinguish between very similar sounds as early as one month after birth and can distinguish between a familiar and non-familiar voice even earlier. Babies who are just a few days old prefer human voices; they will listen to voices longer than sounds that do not involve speech (Vouloumanos & Werker, 2004), and they seem to prefer their mother’s voice over a stranger’s voice (Mills & Melhuish, 1974). In an interesting experiment, 3-week-old babies were given pacifiers that played a recording of the infant’s mother’s voice and of a stranger’s voice. When the infants heard their mother’s voice, they sucked more strongly at the pacifier (Mills & Melhuish, 1974). Some of this ability will be lost by 7 or 8 months as a child becomes familiar with the sounds of a particular language and less sensitive to sounds that are part of an unfamiliar language.
Pain and Touch
Immediately after birth, a newborn is sensitive to touch and temperature and is also sensitive to pain, responding with crying and cardiovascular responses. Newborns who are circumcised (the surgical removal of the foreskin of the penis) without anesthesia experience pain, as demonstrated by increased blood pressure, increased heart rate, decreased oxygen in the blood, and a surge of stress hormones (United States National Library of Medicine, 2016). According to the American Academy of Pediatrics (AAP), there are medical benefits and risks to circumcision. They do not recommend routine circumcision, however, they stated that because of the possible benefits (including prevention from urinary tract infections, penile cancer, and some STIs) parents should have the option to circumcise their sons if they want to (AAP, 2012).
The sense of touch is acute in infants and is essential to a baby’s growth of physical abilities, language and cognitive skills, and socio-emotional competency. Touch not only impacts short-term development during infancy and early childhood but also has long-term effects, suggesting the power of positive, gentle touch from birth. Through touch, infants learn about their world, bond with their caregivers, and communicate their needs and wants. Research emphasizes the great benefits of touch for premature babies, but the presence of such contact has been shown to benefit all children (Stack & Jean, 2011). In an extreme example, some children in Romania were reared in orphanages in which a single care worker may have had as many as 10 infants to care for at one time. These infants were not often helped or given toys with which to play. As a result, many of them were developmentally delayed (Nelson et al., 2014). When we discuss emotional and social development later in this module, you will also see the important role that touch plays in helping infants feel safe and protected, which builds trust and secure attachments between the child and their caregiver.
Taste and Smell
Studies of taste and smell demonstrate that babies respond with different facial expressions, suggesting that certain preferences are innate. Newborns can distinguish between sour, bitter, sweet, and salty flavors and show a preference for sweet flavors.
Infants seem to be born with the ability to perceive the world in an intermodal way, that is, through stimulation from more than one sensory modality. For example, infants who sucked on a pacifier with either a smooth or textured surface preferred to look at a corresponding (smooth or textured) visual model of the pacifier. By 4 months, many infants can match lip movements with speech sounds and can match other audiovisual events. Although sensory development emphasizes the afferent processes used to take in information from the environment, these sensory processes can be affected by the infant’s developing motor abilities. Reaching, crawling, and other actions allow the infant to see, touch, and organize his or her experiences in new ways.
How Infants are Tested
Habituation procedures, that is measuring decreased responsiveness to a stimulus after repeated presentations, have increasingly been used to evaluate infants to study the development of perceptual and memory skills. Phelps (2005) describes a habituation procedure used when measuring the rate of the sucking reflex. Researchers first measure the initial baseline rate of sucking to a pacifier equipped with transducers that measure muscle contractions. Next, an auditory stimulus is presented, such as a human voice uttering a speech sound such as “da.” The rate of sucking will typically increase with the new sound but then decrease to baseline levels as “da” is repeatedly presented, showing habituation. If the sound “ma” was then presented, the rate of sucking would again increase, demonstrating that the infant can discriminate between these two stimuli.
Additionally, the speed or efficiency with which infants show habituation has been shown to predict outcomes in behaviors such as language acquisition and verbal and nonverbal intelligence. Infants who show difficulty during habituation or habituate at slower than normal rates have been found to be at an increased risk for significant developmental delays. Infants with Down syndrome, teratogen-exposed infants, malnourished infants, and premature infants have all been studied. Researchers have found that at the age of 16 months, high-risk infants show rates of habituation comparable to newborn infants (Phelps, 2005).
Sleep and Health
Infant Sleep
Infants 0 to 2 years of age sleep an average of 12.8 hours a day, although this changes and develops gradually throughout an infant’s life. For the first three months, newborns sleep between 14 and 17 hours a day; then, they become increasingly alert for longer periods of time. About one-half of an infant’s sleep is rapid eye movement (REM) sleep, and infants often begin their sleep cycle with REM rather than non-REM sleep. They also move through the sleep cycle more quickly than adults. Parents spend a significant amount of time worrying about and losing even more sleep over their infant’s sleep schedule when there remains a great deal of variation in sleep patterns and habits for individual children. A study by Dias et al. (2018) showed that at 6 months of age, 62% of infants slept at least six hours during the night, 43% of infants slept at least 8 hours through the night, and 38% of infants did not sleep at least six continual hours through the night. At 12 months, 28% of children were still not sleeping at least 6 uninterrupted hours through the night, while 78% were sleeping at least 6 hours, and 56% were sleeping at least 8 hours.
The most common infant sleep-related problem reported by parents is nighttime waking. Studies of new parents and sleep patterns show that parents lose the most sleep during the first three months with a new baby, with mothers losing about an hour of sleep each night and fathers losing a disproportionate 13 minutes. This decline in sleep quality and quantity for adults persists until the child is about six years old.
While this shows there is no precise science as to when and how an infant will sleep, there are general trends in sleep patterns. Around six months, babies typically sleep between 14-15 hours a day, with 3-4 of those hours happening during daytime naps. As they get older, these naps decrease from several to typically two naps a day between ages 9-18 months. Often, periods of rapid weight gain or changes in developmental abilities such as crawling or walking will cause changes to sleep habits as well. Infants generally move towards one 2-4 hour nap a day by around 18 months, and many children will continue to nap until around four or five years old.
Sudden Unexpected Infant Deaths (SUID)
Each year in the United States, there are about 3,400 Sudden Unexpected Infant Deaths (SUID) (Centers for Disease Control and Prevention, 2021). These deaths occur among infants less than one-year-old and have no immediately obvious cause. The three commonly reported types of SUID are:
- Sudden Infant Death Syndrome (SIDS): SIDS is identified when the death of a healthy infant occurs suddenly and unexpectedly, and medical and forensic investigation findings (including an autopsy) are inconclusive. SIDS is the leading cause of death in infants up to 12 months old, and approximately 1,400 infants died of SIDS in 2020 (CDC, 2020). The risk of SIDS is highest at 4 to 6 weeks of age. Because SIDS is diagnosed when no other cause of death can be determined, possible causes of SIDS are regularly researched. One leading hypothesis suggests that infants who die from SIDS have abnormalities in the area of the brainstem responsible for regulating breathing (Weekes-Shackelford & Shackelford, 2005). The idea is that babies die from SIDS because they don’t wake up when they have trouble breathing while sleeping. Although the exact cause is unknown, doctors have identified the following risk factors for SIDS:
-
- low birth weight
- siblings who have had SIDS
- sleep apnea
- of African-American or Eskimo decent
- low socioeconomic status (SES)
- smoking in the home
- Unknown Cause: The sudden death of an infant less than one year of age cannot be explained because a thorough investigation was not conducted, and the cause of death could not be determined.
- Accidental Suffocation and Strangulation in Bed: Reasons for accidental suffocation include: Suffocation by soft bedding, another person rolling on top of or against the infant while sleeping, an infant being wedged between two objects such as a mattress and wall, and strangulation such as when an infant’s head and neck become caught between crib railings.
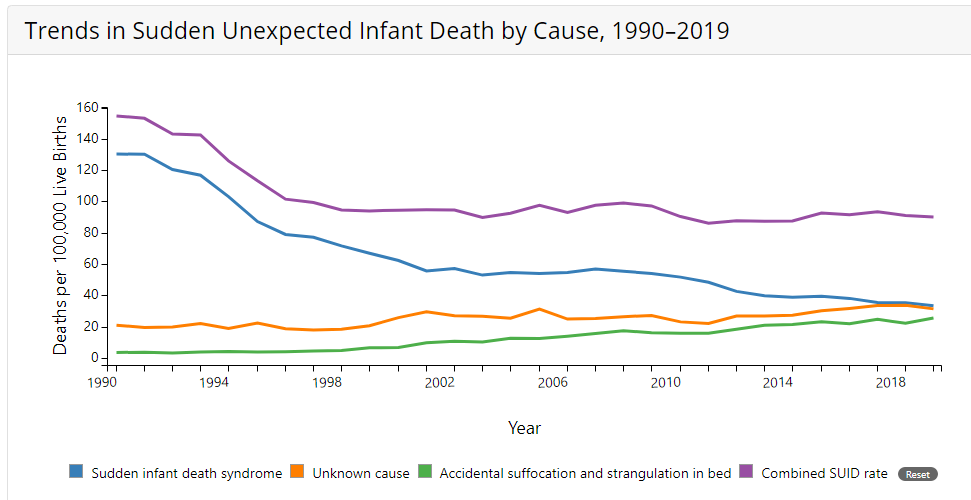
As can be seen in Figure 7, the combined SUID death rate declined considerably in the United States following the release of the American Academy of Pediatrics safe sleep recommendations in 1992. These recommendations advocated that infants be placed for sleep on their backs (nonprone position). These recommendations were followed by a major Back to Sleep Campaign in 1994.
Co-Sleeping
Should infants share the bed with another person? The location of sleep depends primarily on the baby’s age and culture. Bed-sharing (in the parents’ bed) or co-sleeping (in the parents’ room) is the norm in some cultures but not in others (Esposito et al., 2015).
Researchers analyzed a total of 8207 deaths from 24 states during 2004–2012 that were contained in the National Center for the Review and Prevention of Child Deaths Case Reporting System, a database of death reports from state child death review teams (Colvin, et al., 2014). The results indicated that younger victims (0-3 months) were more likely to die by bed-sharing and sleeping in an adult bed/on a person. A higher percentage of older victims (4 months to 364 days) rolled into objects in the sleep environment and changed position from side/back to prone. Investigators compared infants who died of SIDS with a matched control and found that infants younger than three months old who slept in bed with a parent were five times more likely to die of SIDS compared to babies who slept separately from the parents but were still in the same room (Carpenter, et al., 2013).
They concluded that bed-sharing, even when the parents do not smoke or take alcohol or drugs, increases the risk of SIDS. However, when combined with parental smoking and maternal alcohol consumption and/or drug use, risks associated with bed-sharing greatly increased.
Despite the risks noted above, the controversy about where babies should sleep has been ongoing. Co-sleeping has been recommended for those who advocate attachment parenting (Sears & Sears, 2001), and other research suggests that bed-sharing and co-sleeping are becoming more popular in the United States (Colson et al., 2013).
The two studies discussed above were based on American statistics. What about the rest of the world? Co-sleeping occurs in many cultures, primarily because of a more collectivist perspective that encourages a close parent-child bond and interdependent relationship (Morelli, Rogoff, Oppenheim, & Goldsmith, 1992). In countries where co-sleeping is common, however, parents and infants typically sleep on floor mats and other hard surfaces, which minimizes the suffocation that can occur with bedding and mattresses (Nelson et al., 2000).
The American Academy of Pediatrics (AAP) actually updated their recommendations for a Safe Infant Sleeping Environment in 2016. The most recent AAP recommendations on creating a safe sleep environment include:
- Back to sleep for every sleep. Always place the baby on his or her back on a firm sleep surface, such as a crib or bassinet with a tight-fitting sheet.
- Avoid the use of soft bedding, including crib bumpers, blankets, pillows, and soft toys. The crib should be bare.
- Breastfeeding is recommended.
- Share a bedroom with parents, but not the same sleeping surface, preferably until the baby turns 1, but at least for the first six months. Room-sharing decreases the risk of SIDS by as much as 50 percent.
- Avoid the baby’s exposure to smoke, alcohol, and illicit drugs.
As you can see, there is a recommendation to now “share a bedroom with parents,” but not the same sleeping surface. Breastfeeding is also recommended as adding protection against SIDS, but after feeding, the AAP encourages parents to move the baby to his or her separate sleeping space, preferably a crib or bassinet in the parents’ bedroom. Finally, the report included new evidence that supports skin-to-skin care for newborn infants.
Link to Learning
The website Zero to Three has more information on infant sleep patterns, habits, and multiple topics on infancy.
Immunizations
Preventing communicable diseases from early infancy is one of the major tasks of the Public Health System in the USA. Infants mouth every single object they find as one of their typical developmental tasks. They learn through their senses, and tasting objects stimulates their brain and provides a sensory experience as well as learning.
Infants get dirty. They lay on a carpet that most likely has been contaminated by adults walking on it; they mouth keys, rattles, toys, and books; they crawl on the floor; they hold on to furniture to walk, and much more. How do we prevent infants from getting sick? One answer is immunizations. Immunizations are the process by which a person becomes protected against a disease through vaccination (CDC, 2021). Vaccines often contain weakened or inactive parts of a microorganism that prompt the body’s immune system to build up its defenses against the invader.
Many decades ago, our society struggled to find vaccines and cures for illnesses such as Polio, whooping cough, and many other medical conditions. A few decades ago, parents started changing their minds on the need to vaccinate children. Some children are not vaccinated for valid medical reasons, but some states allow a child to be unvaccinated because of a parent’s personal or religious beliefs. At least 1 in 14 children is not vaccinated. What is the outcome of not vaccinating children? Some preventable illnesses are returning. Fortunately, each vaccinated child stops the transmission of the disease, a phenomenon called herd immunity. Usually, if 90% of the people in a community (a herd) are immunized, no one dies or experiences disability from that disease.
In 2017, Community Care Licensing in California, the agency that regulates childcare centers, changed regulations. Before, it was possible for parents to opt out of vaccinations due to personal beliefs, but this changed after Governor Brown signed a Bill in 2016 to only exclude children from being vaccinated if there were medical reasons. Furthermore, all personnel working with children must be immunized. Read more information about vaccinations at the website Shots for School.
COVID-19 Vaccination for Infants
Children aged 6 months to 4 years may need multiple doses of COVID-19 vaccines to be up to date, including at least 1 dose of updated COVID-19 vaccine. This is determined by which vaccine they receive.
Attributions
Human Growth and Development by Ryan Newton is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License,
Individual and Family Development, Health, and Well-being by Diana Lang, Nick Cone; Laura Overstreet, Stephanie Loalada; Suzanne Valentine-French, Martha Lally; Julie Lazzara, and Jamie Skow is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License,
Human Development by Human Development Teaching & Learning Group under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License,
References
Balaban, M. T. & Reisenauer, C. D. (2013). Sensory development. In N. J. Salkind (Ed.), Encyclopedia of human development (pp. 1144-1147). New York: Sage Publications.
Berk, L. (2007). Development through the life span (4th ed.). Boston: Allyn and Bacon.
Berne, S. A. (2006). The primitive reflexes: Considerations in the infant. Optometry & Vision Development, 37(3), 139-145.
Bloem, M. (2007). The 2006 WHO child growth standards. BMJ : British Medical Journal, 334(7596), 705–706.
Carlson, N. (2014). Foundations of behavioral neuroscience (9th ed.). Boston, MA: Pearson.
Carpenter, R., McGarvey, C., Mitchell, E. A., Tappin, D. M., Vennemann, M. M., Smuk, M., & Carpenter, J. R. (2013). Bed sharing when parents do not smoke: is there a risk of SIDS? An individual level analysis of five major case-control studies. BMJ Open, 3(5), e002299. https://doi.org/10.1136/bmjopen-2012-002299
Centers for Disease Control and Prevention. (2021). About SUID and SIDS. https://www.cdc.gov/sids/about/index.htm
Centers for Disease Control and Prevention. (2021). Sudden Unexpected Infant Death and Sudden Infant Death Syndrome – Data and Statistics. https://www.cdc.gov/sids/data.htm
Chi, J. G., Dooling, E. C., & Gilles, F. H. (1977). Left-right asymmetries of the temporal speech areas of the human fetus. Archives of Neurology, 34, 346–8.
Colvin, J.D., Collie-Akers, V., Schunn, C., & Moon, R.Y. (2014). Sleep environment risks for younger and older infants. Pediatrics Online. http://pediatrics.aappublications.org/content/pediatrics/early/2014/07/09/peds. 2014-0401.full.pdf
Dias, C. C., Figueiredo, B., Rocha, M., & Field, T. (2018). Reference values and changes in infant sleep-wake behavior during the first 12 months of life: a systematic review. Journal of sleep research, 27(5), e12654. https://doi.org/10.1111/jsr.12654
Dubois, J., Hertz-Pannier, L., Cachia, A., Mangin, J. F., Le Bihan, D., & Dehaene-Lambertz, G. (2009). Structural asymmetries in the infant language and sensorimotor networks. Cerebral Cortex, 19, 414–423.
Esposito, G., Setoh, P., & Bornstien, M. H. (2015). Beyond practices and values: Toward a physio‑bioecological analysis of sleeping arrangements in early infancy. Frontiers in Psychology, 6. https://hdl.handle.net/10356/107314
El-Dib, M., Massaro, A. N., Glass, P., & Aly, H. (2012). Neurobehavioral assessment as a predictor of neurodevelopmental outcome in preterm infants. Journal of Perinatology, 32, 299-303.
Hutchinson, N. (2011). A geographically informed vision of skills development. Geographical Education, 24, 15.
Huttenlocher, P. R., & Dabholkar, A. S. (1997). Regional differences in synaptogenesis in human cerebral cortex. The Journal of Comparative Neurology, 387(2), 167-178.
Kasprian, G., Langs, G., Brugger, P. C., Bittner, M., Weber, M., Arantes, M., & Prayer, D. (2011). The prenatal origin of hemispheric asymmetry: an in utero neuroimaging study. Cerebral Cortex, 21, 1076–1083.
Kolb, B., & Gibb, R. (2011). Brain plasticity and behaviour in the developing brain. Journal de l’Academie Canadienne de Psychiatrie de l’enfant et de l’adolescent [Journal of the Canadian Academy of Child and Adolescent Psychiatry], 20(4), 265–276
Kolb, B. & Whishaw, I. Q. (2011). An introduction to brain and behavior (3rd ed.). New York: Worth Publishers.
Mills, M., & Melhuish, E. (1974). Recognition of mother’s voice in early infancy. Nature, 252(5479), 123–124. https://doi.org/10.1038/252123a0
Nelson, E. A., Schiefenhoevel, W., & Haimerl, F. (2000). Child care practices in nonindustrialized societies. Pediatrics, 105(6), E75. https://doi.org/10.1542/peds.105.6.e75
Phelps, B. J. (2005). Habituation. In N. J. Salkind (Ed.), Encyclopedia of human development (pp. 597-600). New York: Sage Publications.
Webb, S. J., Monk, C. S., & Nelson, C. A. (2001). Mechanisms of postnatal neurobiological development: Implications for human development. Developmental Neuropsychology, 19, 147-171.
Salkind, N. J. (2005). Encyclopedia of human development. New York: Sage Publications.
Sen, M. G., Yonas, A., & Knill, D. C. (2001). Development of infants’ sensitivity to surface contour information for spatial layout. Perception, 30, 167-176.
Springer, S. P. & Deutsch, G. (1993). Left brain, right brain (4th ed.). New York: W. H. Freeman.
Stack, D. M., & Jean, A. D. L. (2011). Communicating through touch: Touching during parent-infant interactions. In M. J. Hertenstein & S. J. Weiss (Eds.), The handbook of touch: Neuroscience, behavioral, and health perspectives (pp. 273–298). Springer.
Sullivan, R., Perry, R., Sloan, A., Kleinhaus, K., & Burtchen, N. (2011). Infant bonding and attachment to the caregiver: Insights from basic and clinical science. Clinics in Perinatology, 38(4), 643–655. https://doi.org/10.1016/j.clp.2011.08.011
United States National Library of Medicine. (2016). Circumcision. https://medlineplus.gov/circumcision.html
Vouloumanos, A. and Weker, J.F. (2004). Tuned to the signal: the privileged status of speech for young infants. Developmental Science, 7(3) 270-276.
Webb, S. J., Monk, C. S., & Nelson, C. A. (2001). Mechanisms of postnatal neurobiological development: Implications for human development. Developmental Neuropsychology, 19, 147-171. https://www.doi.org/10.1207/S15326942DN1902_2
