Section 6: Early Childhood
6.3 Psychosocial Development in Early Childhood
What are emotional and social developments like in early childhood?
 The time between a child’s second and sixth birthday is full of new social experiences and development. At the beginning of this stage, a child selfishly engages in the world—the goal is to please the self. As children get older, they realize that relationships are built on give-and-take. They typically start to learn to empathize with others and make friends.
The time between a child’s second and sixth birthday is full of new social experiences and development. At the beginning of this stage, a child selfishly engages in the world—the goal is to please the self. As children get older, they realize that relationships are built on give-and-take. They typically start to learn to empathize with others and make friends.
While children are learning about their place in various relationships, they are also developing an understanding of emotion. Two-year-olds do not have a good grasp on their emotions, but by the time they are six, most understand their emotions better. They also understand how to control and mask their emotions—even to the point that they may put on a different emotion than they are actually feeling. By the time children reach six years old, they tend to understand that other people have emotions. They typically develop an understanding that all emotions involved in a situation (theirs and other people’s) should be taken into consideration. That said, although most six-year-olds understand these things, they are not always good at putting the knowledge into action. We’ll examine some of these issues in this section.
Learning Objectives
- Explain Erikson’s stages of psychosocial development for toddlers and children in early childhood.
- Describe the development of a self-concept
- Explain the importance of play
- Summarize theories of gender role development.
- Examine concerns about childhood stress and development.
- Contrast models of parenting styles.
- Examine concerns about childhood stress and trauma, including the concept of ACEs
- Describe the impact of racism on early childhood development
Psychodynamic and Psychosocial Theories of Early Childhood
Freud’s Psychodynamic Theory
Consistent with the sexual development we learned about earlier, Freud asserted that children pass through two stages of his theory during early childhood: stage 2 (anal stage) and stage 3 (phallic stage).
The anal stage begins around 18 months of age and lasts until the child is three years old. During the anal stage, Freud believed that the libido source shifted from the mouth (in stage 1) to the anus. The child, then, receives pleasure from defecating. The child, at this point, understands that they have some amount of control over their lives, including control of when and where they defecate. This can lead to difficulties during potty training. What matters, in terms of Freud’s theory, is how the parent reacts to inevitable difficulties in potty training. Parental reactions during potty training may set up their child to react in one of two ways: (1) parents who are harsh or who ridicule the child for mistakes may have children who stubbornly hold on to their feces in an effort to not have an accident – these children may become anal retentive or (2) parents who are too easy-going may have a child who reacts by purposefully making a mess – these children may become anal expulsive. Adults who are anal retentive tend to be stubborn, very neat, rigid, and stingy. Adults who are anal-expulsive tend to be messy, wasteful, and harsh.
The phallic stage of psychosexual development occurs from ages three to six. According to Freud, during the phallic stage, the child develops an attraction to the opposite-sex parent, which is called the Oedipus Complex for boys and the Electra Complex for girls. When the child recognizes that the opposite-sex parent is unavailable, the child learns to model their own behavior after the same-sex parent. The child develops their own sense of masculinity or femininity from this resolution.
Erikson’s Psychosocial Theory: Initiative vs. Guilt

While Erik Erikson was influenced by Freud, he believed that the relationships that people have, not psychosexual stages, are what influence personality development. At the beginning of early childhood, the child is still in the autonomy versus shame and doubt stage (stage 2).
By age three, the child begins stage 3: initiative versus guilt. The trust and autonomy of previous stages develop into a desire to take initiative or to think of ideas and initiate action (Erikson, 1982). Once children reach the preschool stage (ages 3–6 years), they are capable of initiating activities and asserting control over their world through social interactions and play. According to Erikson, preschool children must resolve the task of initiative vs. guilt. By learning to plan and achieve goals while interacting with others, preschool children can master this task.
Children may want to build a fort with the cushions from the living room couch, open a lemonade stand in the driveway, or make a zoo with their stuffed animals and issue tickets to those who want to come. Or they may just want to get themselves ready for bed without any assistance. Initiative, a sense of ambition and responsibility, occurs when parents allow a child to explore within limits and then support the child’s choice. To reinforce taking initiative, caregivers should offer praise for the child’s efforts and avoid being critical of messes or mistakes. Placing pictures of drawings on the refrigerator, purchasing mud pies for dinner, and admiring towers of legos will facilitate the child’s sense of initiative. These children will develop self-confidence and feel a sense of purpose. Those who are unsuccessful at this stage—with their initiative misfiring or stifled by over-controlling parents—may develop feelings of inadequacy and guilt. Soggy washrags and toothpaste left in the sink pale in comparison to the smiling face of a five-year-old emerging from the bathroom with clean teeth and pajamas!
That said, it is important that caregivers do their best to kindly guide the child to the right actions. Remember that according to Freud and Kohlberg, children are developing a sense of morality during this time. Erikson agrees. If the child does leave those soggy washrags in the sink, have the child help clean them up. It is possible that the child will not be happy with helping to clean, and the child may even become aggressive or angry, but it is important to remember that children are still learning how to navigate their world. They are trying to build a sense of autonomy, and they may not react well when they are asked to do something that they had not planned. Parents should be aware of this and try to be understanding but also firm. The use of gentle parenting, positive discipline, and related consequences will help guide children to positive behaviors. Guilt for a situation where a child did not do their best allows a child to understand their responsibilities and helps the child learn to exercise self-control (remember the marshmallow test). The goal is to find a balance between initiative and guilt, not a free-for-all where the parent allows the child to do anything they want to. Caregivers must guide children if they are to have a successful resolution in this stage.
Video Example
Movies, television, and media, in general, provide many examples of psychosocial development. The movie clips in this video demonstrate Erikson’s third stage of development: initiative versus guilt. What other examples can you think of of young children developing a sense of autonomy?
You can view the transcript for “initiative vs guilt wlmp 2” here (opens in new window).
Developing a Concept of Self
Self Concept
Early childhood is a time of forming an initial sense of self. A self-concept or idea of who we are, what we are capable of doing, and how we think and feel is a social process that involves considering how others view us. It might be said, then, that in order to develop a sense of self, you must interact with others. Interactionist theorists Cooley and Mead offer two interesting explanations of how a sense of self develops.
Cooley’s Looking-Glass Self

Charles Horton Cooley 1964) suggested that our self-concept comes from looking at how others respond to us. This process, known as the looking-glass self, involves looking at how others seem to view us and interpreting this as we make judgments about whether we are good or bad, strong or weak, beautiful or ugly, and so on. Of course, we do not always interpret their responses accurately so our self-concept is not simply a mirror reflection of the views of others. After forming an initial self-concept, we may use our existing self-concept as a mental filter screening out those responses that do not seem to fit our ideas of who we are. So compliments may be negated, for example.
Think of times in your life when you felt more self-conscious. The process of the looking-glass self is pronounced when we are preschoolers. Later in life, we also experience this process when we are in a new school, a new job, or taking on a new role in our personal lives and trying to gauge our own performance. When we feel more positive about who we are, we focus less on how we appear to others.
In summary, self-concept is our self-description according to various categories, such as our external and internal qualities. In contrast, self-esteem is an evaluative judgment about who we are. The emergence of cognitive skills in this age group typically results in improved perceptions of oneself.
Watch this Khan Academy video to learn more about Charles Cooley’s looking-glass self.
Mead’s I and Me
George Herbert Mead (1967) offered an explanation of how we develop a social sense of self by being able to see ourselves through the eyes of others. There are two parts of the self: the “I,” which is the part of the self that is spontaneous, creative, innate, and is not concerned with how others view us, and the “me,” or the social definition of who we are.
When we are born, we are all “I” and act without concern about how others view us. But the socialized self begins when we are able to consider how one important person views us. This initial stage is called “taking the role of the significant other.” For example, a child may pull a cat’s tail and be told by his mother, “No! Don’t do that; that’s bad,” while receiving a slight slap (spanking or slight slapping is not a recommended child-rearing practice) on the hand. Later, the child may mimic the same behavior toward the self and say aloud, “No, that’s bad,” while patting his own hand. What has happened? The child is able to see himself through the eyes of the mother. As the child grows and is exposed to many situations and rules of culture, he begins to view the self in the eyes of many others through these cultural norms or rules. This is referred to as “taking the role of the generalized other” and results in a sense of self with many dimensions. The child comes to have a sense of self as a student, as a friend, as a son, and so on.
Exaggerated Sense of Self
One of the ways to gain a clearer sense of self is to exaggerate those qualities that are to be incorporated into the self. Preschoolers often like to exaggerate their own qualities and seek validation from adults and/or peers. They seek validation, such as if they are the biggest or smartest child or the child who can jump the highest. Much of this may be due to the simple fact that children typically do not understand their own limits. Young children may really believe that they can pick up the refrigerator or win a running race with an Olympic athlete.
This exaggeration tends to be replaced by a more realistic sense of self in middle childhood as children realize that they do have limitations. Part of this process includes having caregivers who allow children to explore their capabilities and give the child authentic feedback. Another important part of this process involves children learning that other people have capabilities, too, and that their own capabilities may differ from those of others.
Emotional self-regulation
Emotional self-regulation refers specifically to an individual’s ability to recognize and name how they are feeling and to express their emotions constructively. Adaptive emotion regulation involves staying in touch with how you are genuinely feeling while at the same time making intentional decisions about how you are going to express those feelings. Three- and four-year-olds learn new ways of expressing their feelings verbally. They also learn how to cope with negative emotions in ways that make themselves feel better—they put their heads down to reduce sensory input that may be overwhelming or unpleasant, they talk out loud to reassure themselves that things will be okay, and they recalibrate their goals or desires to match the options that are available to them, rather than to continue asking for something they cannot have (Thompson & Goodvin, 2007). These strategies, and others, reduce the frequency and severity of tantrums, feelings of loneliness, and other unpleasant emotional responses. They can also help children remain calm when they are very excited or happy.
Self-Control
One important aspect of self-concept is understanding our ability to exhibit self-control and delay gratification. Self-control involves both response inhibition and delayed gratification. Response inhibition involves the ability to recognize a potential behavior before it occurs and stop the initiation of behaviors that could result in undesired consequences. Delayed gratification refers to the process of forgoing immediate or short-term rewards to achieve more valuable goals in the longer term.
One of the places where the developmental task of initiative vs. guilt is negotiated involves preschoolers’ struggles to learn to control their behaviors and emotions. Behavioral self-regulation refers broadly to the self-control individuals use to modify their actions. Sometimes, behaviors need to be modified so that they are socially appropriate to the context (e.g., minding parents or following preschool rules), and sometimes so that they better meet an individual’s own goals (e.g., getting a fort built or joining a pretend game). Adaptive behavioral regulation involves staying in touch with your genuine goals while at the same time making intentional decisions about the actions you are going to show in service of those goals.
Self‐regulation of behavior refers to both:
- “Do” regulation: The performance of actions desired by others that we don’t really want to do (“Put away your toys”), and
- “Don’t” regulation: Stopping ourselves from doing something we really want to do (“Don’t eat that cookie!”).
During toddlerhood, we see the start of behavioral self-regulation, and it is one of the central tasks of early childhood, but these processes take many years to fully develop. Executive function refers to self-regulatory processes, such as the ability to inhibit behavior or cognitive flexibility, that enable adaptive responses to new situations or to reach a specific goal. Executive function skills gradually emerge during early childhood and continue to develop throughout childhood and adolescence. Like many cognitive changes, brain maturation, especially the prefrontal cortex, along with experience, influences the development of executive function skills. As executive function improves, children become less impulsive (Traverso, Viterbori, & Usai, 2015). Children show higher executive function skills when parents are warm and responsive, use scaffolding when the child is trying to solve a problem and provide cognitively stimulating environments (Fay-Stammbach, Hawes & Meredith, 2014).
When do children start self-regulating, and what affects how it develops? Children start regulating their behaviors in infancy, beginning with physiological regulation and consistency in patterns of behavior, such as sleeping and eating. However, as infants move into toddlerhood, they are faced with the challenge of regulating their behavior as it relates to others in social situations. This type of self-regulation is typically not seen with any degree of consistency until a child’s second year. However, the capacity to self-regulate may develop earlier or later depending on:
- Developmental progress in other areas, such as cognition and working memory, helps children become aware of what constitutes acceptable social behavior.
- The child’s temperament, both reactivity and effortful control.
- The quality of parent-child interactions.
- The quality of the general home and/or school (day-care) environment.
Why is self-regulation important? Being good at behavioral self-regulation (compared to having difficulty regulating one’s behavior) is associated with numerous positive outcomes for children, including:
- More success in the transition to school and better academic achievement once they start school.
- Higher levels of social competence are seen in greater success in developing school-based peer relationships.
- Fewer problems with externalizing behaviors such as anger and impulsivity.
- There are higher levels of prosocial behaviors as children move from infancy into toddlerhood and early childhood and increases in prosocial behavior throughout childhood.
While self-control takes many years to develop, we typically see the beginnings of this skill during early childhood. This ability to delay gratification in young children was thought to predict many positive outcomes. The ability to delay gratification was traditionally assessed in young children with the “Marshmallow Test” (Mischel, Ebbesen, & Zeiss, 1972). During this experiment, participants were presented with a marshmallow (or another small treat) and were given a choice to eat it or wait for a certain period of time without eating it so that they could have two marshmallows. Michel et al. (2011) found that preschoolers who were able to delay gratification for a longer period of time had higher levels of resilience, better academic and social competence, and greater planning ability in their adolescence.
However, Watts et al. (2018) replication of the Marshmallow Test, originally conducted by Walter Mischel in the 1960s, aimed to assess whether the ability to delay gratification still correlated with long-term academic and behavioral outcomes. This replication involved more diverse samples to account for socioeconomic and cultural factors, revealing that while self-control is a significant predictor of future success, environmental influences, socioeconomic status, and upbringing play crucial roles as well.
In 2024, the Watts et al. (2018) research was replicated by Sperber et al. (2024), and the results indicate that Marshmallow Test performance does not reliably predict adult outcomes supporting the idea that multiple factors influence the development of self-regulation.
This video explains Mead’s understanding of the “I” and the “me,” and compares it to other concepts you’ve already learned about, like egocentrism.
You may know about The Marshmallow Test, a popular psychological exam to see if people have willpower, but psychologists found that it might not be measuring willpower after all. A replication of this research found that the marshmallow test could not predict adult outcomes (Sperber et al., 2024)
Think about it:
Recent research has found that environmental factors, including socioeconomic level, influence success at a delay of gratification task. Why do you think that is?
Social Development: The Importance of Play

The development of play is an important milestone in early childhood. Play holds a crucial role in providing a safe, caring, protective, confidential, and containing space where children can recreate themselves and their experiences through an exploratory process (Winnicott, 1942; Erikson, 1963). During this stage, pretend play is a great way for children to express their thoughts, emotions, fears, and anxieties. One type of pretend play is sociodramatic play, where children imitate adults and take on adult roles and activities, like playing house or doctor. Vygotsky saw sociodramatic play as fuel for cognitive, social, and emotional development, and research confirmed it showing sociodramatic play predicted better self-regulation in 3- and 4-year-olds (Elias & Berk, 2002).
Another important type of pretend play is rough and tumble play or play fighting, wrestling, and chasing. Commonly seen in rats, monkeys, and other mammals, rough-and-tumble play is believed to be an evolutionary adaptation that helps build the social brain (Pellis and Pellis, 2007). It’s more frequent and rough in boys. It is associated with human social competence. Rough and tumble play is different than real fighting as the participants are often laughing and taking care not to harm each other. It helps children learn restraint and impulse control.
Early childhood play can be understood by observing the elements of fantasy, organization, and comfort. Fantasy, the process of make-believe, is an essential behavior the child engages in during pretend play; organization helps the child structure pretend play into a story and utilize cause-and-effect thinking, and comfort is used to assess the ease and pleasure of the engagement in play.
As children progress through the stage of early childhood, they also progress through several stages of non-social and social play. Stages of play is a theory and classification of participation in play developed by Mildred Parten Newhall in 1929 (Hughes, 2009). Parten observed American children at free play. She recognized six different types of play:
|
Unoccupied Play |
Children’s behavior seems more random and without a specific goal. This is the least common form of play. |
|---|---|
|
Solitary Play |
Children play by themselves, do not interact with others, nor are they engaging in similar activities as the children around them. |
|
Onlooker Play |
Children are observing other children playing. They may comment on the activities and even make suggestions, but will not directly join the play. |
|
Parallel Play |
Children play alongside each other, using similar toys, but do not directly act with each other. |
|
Associative Play |
Children will interact with each other and share toys, but are not working toward a common goal. |
|
Cooperative Play |
Children are interacting to achieve a common goal. Children may take on different tasks to reach that goal. |
EVERYDAY CONNECTION: The Importance of Play and Recess
According to the American Academy of Pediatrics (2007), unstructured play is an integral part of a child’s development. It builds creativity, problem-solving skills, and social relationships. Play also allows children to develop a theory of mind as they imaginatively take on the perspective of others.
Outdoor play allows children the opportunity to directly experience and sense the world around them. While doing so, they may collect objects that they come across and develop lifelong interests and hobbies. They also benefit from increased exercise, and engaging in outdoor play can actually increase how much they enjoy physical activity. This helps support the development of a healthy heart and brain. Unfortunately, research suggests that today’s children are engaging in less and less outdoor play (Clements, 2004). Perhaps, it is no surprise to learn that lowered levels of physical activity in conjunction with easy access to calorie-dense foods with little nutritional value are contributing to alarming levels of childhood obesity (Karnik & Kanekar, 2012).
Despite the adverse consequences associated with reduced play, some children are overscheduled and have little free time to engage in unstructured play. In addition, some schools have taken away recess time for children in a push to get students to do better on standardized tests, and many schools commonly use the loss of recess as a form of punishment.
Do you agree with these practices? Why or why not?
Gender Identity, Gender Constancy, and Gender Roles
Another important dimension of the self is the sense of self as male or female. Preschool-aged children become increasingly interested in finding out the differences between boys and girls, both physically and in terms of what activities are acceptable for each. While two-year-olds can identify some differences and learn whether they are boys or girls, preschoolers become more interested in what it means to be male or female. This self-identification, or gender identity, is followed sometime later with gender constancy, or the understanding that superficial changes do not mean that gender has actually changed. For example, if you are playing with a two-year-old boy and put barrettes in his hair, he may protest, saying that he doesn’t want to be a girl. By the time a child is four years old, they have a solid understanding that putting barrettes in their hair does not change their gender.
Children learn at a young age that there are distinct expectations for boys and girls. Cross-cultural studies reveal that children are aware of gender roles by age two or three. At four or five, most children are firmly entrenched in culturally appropriate gender roles (Kane 1996). Children acquire these roles through socialization, a process in which people learn to behave in a particular way as dictated by societal values, beliefs, and attitudes.
Children may also use gender stereotyping readily. Gender stereotyping involves overgeneralizing the attitudes, traits, or behavior patterns of women or men. A recent research study examined four- and five-year-old children’s predictions concerning the sex of the persons carrying out a variety of common activities and occupations on television. The children’s responses revealed strong gender-stereotyped expectations. They also found that children’s estimates of their own future competence indicated stereotypical beliefs, with the females more likely to reject masculine activities.
Children who are allowed to explore different toys, who are exposed to non-traditional gender roles, and whose parents and caregivers are open to allowing the child to take part in non-traditional play (allowing a boy to nurture a doll or allowing a girl to play doctor) tend to have broader definitions of what is gender appropriate and may do less gender stereotyping.
This clip from Upworthy shows how some children were surprised to meet women in traditionally male occupations.
The National Center on Parent, Family, and Community Engagement identified several stages of gender identity development, as outlined below. You can see more of their resources and tips for healthy gender development by reading Healthy Gender Development and Young Children.
- Infancy. Children observe messages about gender from adults’ appearances, activities, and behaviors. Most parents’ interactions with their infants are shaped by the child’s gender, and this in turn also shapes the child’s understanding of gender (Fagot & Leinbach, 1989; Witt, 1997; Zosuls et al., 2011).
- 18–24 months. Toddlers begin to define gender, using messages from many sources. As they develop a sense of self, toddlers look for patterns in their homes and early care settings. Gender is one way to understand group belonging, which is important for secure development (Kuhn et al., 1978; Langlois & Downs, 1980; Fagot & Leinbach, 1989; Baldwin & Moses, 1996; Witt, 1997; Antill et al., 2003; Zosuls et al., 2009).
- Ages 3–4. Gender identity takes on more meaning as children begin to focus on all kinds of differences. Children begin to connect the concept “girl” or “boy” to specific attributes. They form stronger rules or expectations for how each gender behaves and looks (Kuhn et al., 1978; Martin et al., 2004; Halim & Ruble, 2010).
- Ages 5–6. At these ages, children’s thinking may be rigid in many ways. For example, 5- and 6-year-olds are very aware of rules and of the pressure to comply with them. They do so rigidly because they are not yet developmentally ready to think more deeply about the beliefs and values that many rules are based on. For example, as early educators and parents know, the use of “white lies” is still hard for them to understand. Researchers call these ages the most “rigid” period of gender identity. (Weinraub et al., 1984; Egan et al., 2001; Miller et al., 2009). A child who wants to do or wear things that are not typical of his gender is probably aware that other children find it strange. The persistence of these choices, despite the negative reactions of others, shows that these are strong feelings. Gender rigidity typically declines as children age (Trautner et al., 2005; Halim, et al., 2013). With this change, children develop stronger moral impulses about what is “fair” for themselves and other children (Killen & Stangor, 2001).
It is important to understand these typical and normal attempts for children to understand the world around them. It is helpful to encourage children and support them as individuals instead of emphasizing or playing into gender roles and expectations. You can foster self-esteem in children of any gender by giving all children positive feedback about their unique skills and qualities. For example, you might say to a child, “I noticed how kind you were to your friend when she fell down,” or “You were very helpful with clean-up today—you are such a great helper,” or “You were such a strong runner on the playground today.”
Learning Through Reinforcement and Modeling
Learning theorists suggest that gender role socialization largely comes from operant conditioning (reinforcement or punishment) and social learning; it is a result of the ways in which parents, teachers, friends, schools, religious institutions, media, and others send messages about what is acceptable or desirable behavior for males or females. This socialization begins early—in fact, it may even begin the moment a parent learns that a child is on the way. Knowing the sex of the child can conjure up images of the child’s behavior, appearance, and potential on the part of a parent. And this stereotyping continues to guide perception through life. Consider parents of newborns. Shown a 7-pound, 20-inch baby, wrapped in blue (a color designating males), parents described the infant as “tough, strong, and angry” when crying. Shown the same infant in pink (a color used in the U.S. for baby girls), these same parents describe the baby as “pretty, delicate, and frustrated” when crying (Maccoby & Jacklin, 1987). Female infants are held more, talked to more frequently, and given direct eye contact, while male infants’ play is often with toys or activities.
One way children learn gender roles is through play. Parents typically supply boys with trucks, toy guns, and superhero paraphernalia, which are active toys that promote motor skills, aggression, and solitary play. Daughters are often given dolls and dress-up apparel that foster nurturing, social proximity, and role play. Studies have shown that children will most likely choose to play with “gender appropriate” toys (or same-gender toys) even when cross-gender toys are available because of operant conditioning: parents positively reinforce children with feedback (in the form of praise, involvement, and physical closeness) for gender normative behavior (Caldera et al., 1998).

Sons are given tasks that take them outside the house and that have to be performed only on occasion, while girls are more likely to be given chores inside the home, such as cleaning or cooking, that are performed daily. Sons are encouraged to think for themselves when they encounter problems, and daughters are more likely to be given assistance even when they are working on an answer. This impatience is reflected in teachers waiting less time when asking a female student for an answer than when asking for a reply from a male student (Sadker and Sadker, 1994). Girls are given the message from teachers that they must try harder and endure in order to succeed, while boys’ successes are attributed to their intelligence. Of course, the stereotypes of advisors can also influence which kinds of courses or vocational choices girls and boys are encouraged to make.
Social learning is also key. Friends discuss what is acceptable for boys and girls, and popularity may be based on modeling what is considered ideal behavior or appearance for the sexes. Girls tend to tell one another secrets to validate others as best friends, while boys compete for position by emphasizing their knowledge, strength, or accomplishments. This focus on accomplishments can even give rise to exaggerating accomplishments in boys, but girls are discouraged from showing off and may learn to minimize their accomplishments as a result.
Gender messages abound in our environment. But does this mean that each of us receives and interprets these messages in the same way? Probably not. From a cognitive perspective, how children think about gender differs as kids develop their own gender schema or mental categories about gender (Bem, 1981). In addition to being recipients of these cultural expectations, we are individuals who also modify these roles (Kimmel, 2008).
One interesting recent finding is that girls may have an easier time breaking gender norms than boys. Girls who play with masculine toys often do not face the same ridicule from adults or peers that boys face when they want to play with feminine toys. Girls also face less ridicule when playing a masculine role (like doctor) than boys who want to take a feminine role (like caregiver).
This video provides an overview of common toy commercials and how they can be analyzed based on recent research on gender stereotypes. What gender roles or gender stereotypes have you noticed in toy commercials? How do you think toy commercials have changed over the past few years?
You can view the transcript for “Toy Commercials: Playing with Gender” here (opens in new window).
The Impact of Gender Discrimination
How much does gender matter? In the United States, gender differences are found in school experiences. Even in college and professional school, girls are less vocal in class and much more at risk for sexual harassment from teachers, coaches, classmates, and professors. These gender differences are also found in social interactions and in media messages. The stereotypes that boys should be strong, forceful, active, dominant, and rational and that girls should be pretty, subordinate, unintelligent, emotional, and talkative are portrayed in children’s toys, books, commercials, video games, movies, television shows, and music. In adulthood, these differences are reflected in income gaps between men and women (women working full-time earn about 74 percent of the income of men), in higher rates of women suffering rape and domestic violence, higher rates of eating disorders for females, and in higher rates of violent death for men in young adulthood.
Gender differences in India can be a matter of life and death as preferences for male children have been historically strong and are still held, especially in rural areas (WHO, 2010). Male children are given preference for receiving food, breast milk, medical care, and other resources. In some countries, it is no longer legal to give parents information on the sex of their developing child for fear that they will abort a female fetus. Clearly, gender socialization and discrimination still impact development in a variety of ways across the globe. Gender discrimination generally persists throughout the lifespan in the form of obstacles to education or lack of access to political, financial, and social power.
Family Factors: Parenting Styles
Relationships between parents and children continue to play a significant role in children’s development during early childhood. As children mature, parent-child relationships naturally change. Preschool and grade-school children are more capable, have their own preferences, and sometimes refuse or seek to compromise with parental expectations. This can lead to greater parent-child conflict, and how conflict is managed by parents further shapes the quality of parent-child relationships. The parenting style used to rear a child will likely impact that child’s future success in romantic, peer, and parenting relationships.
Diana Baumrind’s Parenting Styles
Baumrind (1971) identified a model of parenting that focuses on the level of control/ expectations that parents have regarding their children and how warm/responsive they are. Baumrind, a clinical and developmental psychologist, coined the following parenting styles: authoritative, authoritarian, and permissive/indulgent. Later, Maccoby and Martin added the uninvolved/neglectful style.

It is beneficial to evaluate the support and demandingness of a caregiver in order to determine which style is being used and how to effectively use it. Support refers to the amount of affection, acceptance, and warmth a parent provides to a child. Demandingness refers to the degree a parent controls a child’s behavior.
Authoritative Parenting. In general, children tend to develop greater competence and self-confidence when parents have high but reasonable and consistent expectations for children’s behavior, communicate well with them, are warm and responsive, and use reasoning rather than coercion to guide children’s behaviors. This kind of parenting style has been described as authoritative. (Baumrind, 2013). Authoritative parents are supportive and show interest in their kids’ activities but are not overbearing and allow children to make constructive mistakes. This “tender teacher” approach is deemed the most optimal parenting style to use in Western cultures. Children whose parents use the authoritative style are generally happy, capable, and successful (Maccoby, 1992).

Authoritarian Parenting. Authoritarian is the traditional model of parenting in which parents make the rules and children are expected to be obedient. Parents using the authoritarian (“rigid ruler”) approach are low in support and high in demandingness. These parents expect and demand obedience because they are “in charge,” and they do not provide any explanations for their orders (Baumrind, 1991). Parents also provide well-ordered and structured environments with clearly stated rules.
Many would conclude that this is the parenting style used by Harry Potter’s harsh aunt and uncle and Cinderella’s vindictive stepmother. Consequently, children reared in this way may fear rather than respect their parents and, because their parents do not allow discussion, may take out their frustrations on safer targets-perhaps as bullies toward peers. Children reared in environments using the authoritarian approach are more likely to be obedient and proficient but score lower in happiness, social competence, and self-esteem.
Permissive Parenting. Permissive parenting involves holding expectations of children that are below what could be reasonably expected from them. Parents who are high in support and low in demandingness are likely using the permissive-also called the indulgent-style. Their children tend to rank low in happiness and self-regulation and are more likely to have problems with authority. Parents using this approach are lenient, do not expect their children to adhere to boundaries or rules, and avoid confrontation (Baumrind, 1991). Children fail to learn self-discipline and may feel somewhat insecure because they do not know the limits.
Uninvolved Parenting. Children reared by parents who are low in both support and demandingness tend to rank lowest across all life domains, lack self-control, have low self-esteem, and are less competent than their peers. Parents using the uninvolved (or sometimes referred to as indifferent or neglectful) approach are neglectful or rejecting of their children and do not provide most, if any, necessary parenting responsibilities.
Keep in mind that most parents do not follow any model completely. Real people tend to fall somewhere in between these styles. Sometimes parenting styles change from one child to the next or in times when the parent has more or less time and energy for parenting. Parenting styles can also be affected by concerns the parent has in other areas of his or her life. For example, parenting styles tend to become more authoritarian when parents are tired and perhaps more authoritative when they are more energetic. Sometimes parents seem to change their parenting approach when others are around, maybe because they become more self-conscious as parents or are concerned with giving others the impression that they are a “tough” parent or an “easy-going” parent. Additionally, parenting styles may reflect the type of parenting someone saw modeled while growing up.
Culture. The impact of culture and class cannot be ignored when examining parenting styles. The model of parenting described above assumes that the authoritative style is the best because this style is designed to help the parent raise a child who is independent, self-reliant, and responsible. These are qualities favored in “individualistic” cultures such as the United States, particularly by the middle class. However, in “collectivistic” cultures such as China or Korea, being obedient and compliant are favored behaviors. Authoritarian parenting has been used historically and reflects the cultural need for children to do as they are told. African-American, Hispanic, and Asian parents tend to be more authoritarian than non-Hispanic whites. In societies where family members’ cooperation is necessary for survival, rearing children who are independent and who strive to be on their own makes no sense. However, in an economy based on being mobile in order to find jobs and where one’s earnings are based on education, raising a child to be independent is very important.
In a classic study on social class and parenting styles, Kohn (1977) explains that parents tend to emphasize qualities that are needed for their own survival when parenting their children. Working-class parents are rewarded for being obedient, reliable, and honest in their jobs. They are not paid to be independent or to question the management; rather, they move up and are considered good employees if they show up on time, do their work as they are told, and can be counted on by their employers. Consequently, these parents reward honesty and obedience in their children. Middle-class parents who work as professionals are rewarded for taking the initiative, being self-directed, and being assertive in their jobs. They are required to get the job done without being told exactly what to do. They are asked to be innovative and to work independently. These parents encourage their children to have those qualities as well by rewarding independence and self-reliance. Parenting styles can reflect many elements of culture.
Watch about Baumrind’s parenting styles
Parenting Styles and Outcomes for Children
Parenting style has been found to predict child well-being in the domains of social competence, academic performance, psychosocial development, and problem behavior. Research in the United States, based on parent interviews, child reports, and parent observations, consistently finds:
- Children and adolescents whose parents use the authoritative style typically rate themselves and are rated by objective measures as more socially and instrumentally competent than those whose parents do not use the authoritative style (Baumrind, 1991; Weiss & Schwarz, 1996; Miller et al., 1993).
- Children and adolescents whose parents are uninvolved typically perform most poorly in all domains.
In general, parental responsiveness tends to predict social competence and psychosocial functioning, while parental demandingness is typically associated with instrumental competence and behavioral control (e.g., academic performance and deviance). These findings indicate:
- Children and adolescents reared in households using the authoritarian style (high in demandingness but low in responsiveness) tend to perform moderately well in school and be uninvolved in problem behavior but tend to have poorer social skills, lower self-esteem, and higher levels of depression when compared to their peers who are reared in households using the authoritative approach.
- Children and adolescents reared in homes using the indulgent style (high in responsiveness, low in demandingness) tend to be more involved in problem behavior and perform less well in school, but they have been shown to have higher self-esteem, better social skills and lower levels of depression when compared to their peers who are not reared using the indulgent style (Darling, 1999).
| Support (Low) | Support (High) | |
| Demand (Low) | Uninvolved | Permissive |
| Demand (High | Authoritarian | Authoritative |
In reviewing the literature on parenting styles, it is apparent that using the authoritative parenting style is associated with both instrumental and social competence and lower levels of problem behavior at all developmental stages for youth in the United States. The benefits of using the authoritative parenting style and the detrimental effects of the uninvolved parenting style are evident as early as the preschool years and continue throughout adolescence and into early adulthood.
Support for Baumrind’s Authoritative Parenting
Support for the benefits of authoritative parenting has been found in countries as diverse as the Czech Republic (Dmitrie et al., 2004). India (Carson et al., 1999), China (Pilgrim et al., 1999), Israel (Mayseless et al., 2003), and Palestine (Punaet al., 1997). In fact, authoritative parenting appears to be superior in Western, individualistic societies—so much so that some people have argued that there is no longer a need to study it (Steinberg, 2001).
Other researchers are less certain about authoritative parenting and point to differences in cultural values and beliefs. For example, while many children reared in European-American cultures fare poorly with too much strictness (authoritarian parenting), children reared in Chinese cultures often perform well, especially academically. The reason for this likely stems from Chinese culture viewing strictness in parenting as related to training, which is not central to American parenting beliefs. (Chao, 1994).
As children mature, parent-child relationships should naturally adapt to accommodate developmental changes. Parent-child relationships that do not adapt to a child’s abilities can lead to high parent-child conflict and, ultimately, a reduced parent-child relationship quality.
Stress in Early Childhood

What is the impact of stress on child development? The answer is complex and depends on several factors, including the number of stressors, the duration of stress, and the child’s ability to cope with stress.
Children experience different types of stressors that could be manifest in various ways. Normal, everyday stress can provide an opportunity for young children to build coping skills and poses little risk to development. Even long-lasting stressful events, such as changing schools or losing a loved one, can be managed fairly well.
Some experts have theorized that there is a point where prolonged or excessive stress becomes harmful and can lead to serious health effects. When stress builds up in early childhood, neurobiological factors are affected; in turn, levels of the stress hormone cortisol exceed normal ranges. Due in part to the biological consequences of excessive cortisol, children can develop physical, emotional, and social symptoms. Physical conditions include cardiovascular problems, skin conditions, susceptibility to viruses, headaches, or stomach aches in young children. Emotionally, children may become anxious or depressed, violent, or feel overwhelmed. Socially, they may become withdrawn and act out toward others or develop new behavioral ticks such as biting nails or picking at skin.
Types of Stress
Researchers have proposed three distinct types of responses to stress in young children: positive, tolerable, and toxic. Positive stress (also called eustress) is necessary and promotes resilience, or the ability to function competently under threat. Such stress arises from brief, mild to moderate stressful experiences, buffered by the presence of a caring adult who can help the child cope with the stressor. This type of stress causes minor, temporary physiological and hormonal changes in the young child, such as an increase in heart rate and a change in hormone cortisol levels. The first day of school, a family wedding, or making new friends are all examples of positive stressors. Tolerable stress comes from adverse experiences that are more intense in nature but short-lived and can usually be overcome. Some examples of tolerable stressors are family disruptions, accidents, or the death of a loved one. The body’s stress response is more intensely activated due to severe stressors; however, the response is still adaptive and temporary.
Toxic stress is a term coined by pediatrician Jack P. Shonkoff of the Center on the Developing Child at Harvard University to refer to chronic, excessive stress that exceeds a child’s ability to cope, especially in the absence of supportive caregiving from adults. Extreme, long-lasting stress in the absence of supportive relationships to buffer the effects of a heightened stress response can produce damage and weakening of bodily and brain systems, which can lead to diminished physical and mental health throughout a person’s lifetime. Exposure to such toxic stress can result in the stress response system becoming more highly sensitized to stressful events, producing increased wear and tear on physical systems through over-activation of the body’s stress response. This wear and tear increases the later risk of various physical and mental illnesses.
Consequences of Toxic Stress
Children who experience toxic stress or who live in extremely stressful situations of abuse over long periods of time can suffer long-lasting effects. The structures in the midbrain or limbic system, such as the hippocampus and amygdala, can be vulnerable to prolonged stress (Middlebrooks & Audage, 2008). High levels of the stress hormone cortisol can reduce the size of the hippocampus and affect a child’s memory abilities. Stress hormones can also reduce immunity to disease. If the brain is exposed to long periods of severe stress, it can develop a low threshold, making a child hypersensitive to stress in the future.
With chronic toxic stress, children undergo long-term hyper-arousal of brain stem activity. This includes an increase in heart rate, blood pressure, and arousal states. These children may experience a change in brain chemistry, which leads to hyperactivity and anxiety. Therefore, it is evident that chronic stress in a young child’s life can create significant physical, emotional, psychological, social, and behavioral changes; however, the effects of stress can be minimized if the child has the support of caring adults.
This short video explains some of the biological changes that accompany toxic stress.
You can view the transcript for “3. Toxic Stress Derails Healthy Development” here (opens in new window).
Coping with Stress
Stress has four different stages. In the first stage, it usually causes alarm. Next, in the second or appraisal stage, the child attempts to find meaning from the event. Stage three consists of children seeking out coping strategies. Lastly, in stage four, children execute one or more of the coping strategies. However, children with a lower tolerance for stressors are more susceptible to alarm and find a broader array of events to be stressful. These children often experience chronic or toxic stress.
Managing Stress
Some recommendations to help children manage stressful situations include:
- Preparing children for everyday stressful situations, such as traveling to new places or going to the doctor. For example, talk to children about the experience to help them understand that it is okay to be stressed and scared.
- Keeping communication open. This includes making sure that the child feels comfortable talking to a person. This may include being in a comfortable space, such as their bedroom, where they feel safe. The comfort level of the child is important because if a child is not comfortable, or feels forced to speak, they may not open up at all.
- Spending time together as a family so that no one’s feelings go unseen; ensuring that a child knows that their feelings are valued, and should be expressed in healthy ways.
- Modeling healthy and successful coping mechanisms (such as going for a walk).
- Encouraging children to express themselves creatively (as an outlet or to help others to understand what is stressing the child). Some healthy outlets of stress-relief include sports or running, writing, reading, art, as well as playing musical instruments.
- Teaching children to act and think positively when they are faced with a situation to manage the stress before it becomes overwhelming.
- Providing a safe and healthy home and environment for children.
- Providing children with proper nutrition and attention.
- Ensuring children are not exposed to substance abuse or violence. When a healthy environment is provided, children are more likely to be emotionally and physically healthy
This video describes a variety of factors involved in the development of resilience.
You can view the transcript for “InBrief: The Science of Resilience” here (opens in new window).
Racism in Early Childhood
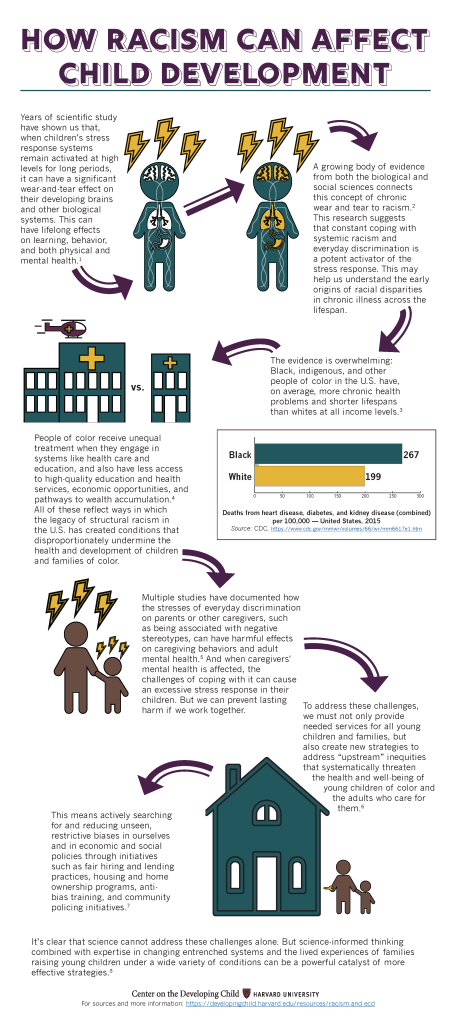
Recent research on the impact of racism on early childhood development reveals significant and long-lasting effects on both physical and mental health. Here’s a summary of key findings:
- Biological and Brain Development: Studies (Harvard Center on the Developing Child, 2023; McLean Hospital, 2023) have shown that exposure to racism, whether structural or interpersonal, can lead to toxic stress in children, which adversely affects brain development. Research using brain imaging has found that children who experience high levels of racial stress tend to have reduced gray matter volume in critical brain regions like the prefrontal cortex and amygdala. These areas are essential for emotional regulation, learning, and memory. The stress associated with racism can predispose children to mental health disorders, such as PTSD, even at a young age.
- Health and Well-being: Prolonged exposure to racism and discrimination contributes to the activation of chronic stress responses, which can lead to long-term health problems (Harvard Center on the Developing Child, 2023). These include increased risks of cardiovascular diseases, weakened immune systems, and higher rates of anxiety and depression. The Harvard Center on the Developing Child (2023) emphasizes that the stress from racism can disrupt the foundational health and development of children, particularly when it occurs during critical developmental periods.
- Social and Emotional Impact: Racism in early life affects children’s social interactions and emotional health. It can lead to feelings of inferiority, social withdrawal, and difficulties in forming healthy relationships. For Black children, experiences of racism are often compounded by other forms of discrimination, further exacerbating the impact on their development. Studies have also highlighted how these effects can differ based on gender and other intersecting identities, showing that the impact of racism is multifaceted and complex.
- Interventions and Policy Recommendations: To mitigate these adverse effects, researchers advocate for early interventions that support children and families experiencing racism. These interventions include creating supportive educational environments, providing mental health resources, and addressing systemic inequalities through policy changes. By focusing on building resilience and reducing exposure to racism, it is possible to improve long-term outcomes for affected children Harvard Center on the Developing Child, 2023.)
Trauma in Childhood
Adverse Childhood Experiences (ACEs)
Over the last 20 years, a framework has become popular that gathers up a variety of sources of early stress and considers them together as adverse childhood experiences (or ACEs; CDC, 2019; Merrick, Ford, Ports, & Guinn, 2018; Petruccelli, Davis, & Berman, 2019). This area of study was initiated when researchers created a scale that listed the most common of these early developmental risks (i.e., neglect; verbal, physical, and sexual abuse; and family dysfunction based on mental health, substance abuse, and domestic violence) and asked adults to report whether they had experienced any of them before they turned 18. Researchers then counted the number of experiences (creating an index of cumulative risk) and examined whether people with different numbers of ACEs also showed differences in physical or psychological functioning. This line of work revealed two things: ACEs are common– about 70% of adults have experienced at least one, and 25% at least three. The number of ACEs, especially when it reaches 4 or more, is a strong predictor of a range of psychological and physical health problems. Researchers sometimes even estimate the cost of ACEs in the number of years they subtract from a person’s average life expectancy.
By drawing together events as diverse as maternal death and physical abuse, researchers have learned that these experiences tend to co-occur and that their effects are cumulative. This means, for example, that intimate partner violence is often accompanied by maternal depression, neglect, and physical abuse, and it is this combination of events that takes its toll. This suggests that it is not possible to understand the effects of any one adverse experience without considering the entire profile to which a child has been exposed. The more chronic and widespread the experiences, the more serious their impact on development.
Moreover, an overarching framework has allowed researchers who study different kinds of adversity to realize that many of these early experiences influence subsequent development through a common set of pathways. Many of these experiences interfere with the healthy development of the neurophysiological systems that deal with stress. The two primary pathways through which early adversity registers in long-term health effects seem to be (1) increases in behavioral risk, in which changes in brain systems render individuals more susceptible to substance abuse and other behaviors that pose health risks; and (2) over and above the effects of risky behaviors, early insult to the immune and other biological system leads to greater vulnerability to health conditions later in life (e.g., cardiovascular disease, cancer, diabetes, and autoimmune conditions like asthma).
Neurophysiological effects of early adversity. The stress systems that govern “fight-flight-or-freeze” responses are complex and involve the endocrine and immune systems; the centers of the brain that regulate fear (e.g., the amygdala), pleasure (e.g., the nucleus accumbens), and memory (e.g., the hippocampus); and the brain areas that serve intentional self-regulation, decision-making, and planning. (i.e., the prefrontal cortex). When children are chronically overwhelmed by stress, the healthy development of all of these neurobiological systems can be compromised, often at the epigenetic level. An impaired stress regulation system interferes broadly with normal cognitive, social, emotional, and physical development and may even undermine long-term psychological and physical health and functioning.
ACEs are found across all demographic groups, but as you might expect from readings on higher-order contexts, those who are low-income or de-valued by society may be at higher risk: A study by Merrick and colleagues (2018) found significantly higher ACE exposure for those who identified as Black, multiracial, lesbian/gay/bisexual, or reported being low income or unemployed or having less than a high school education.
To determine your own ACEs score, visit this website to take the Adverse Childhood Experiences Quiz.
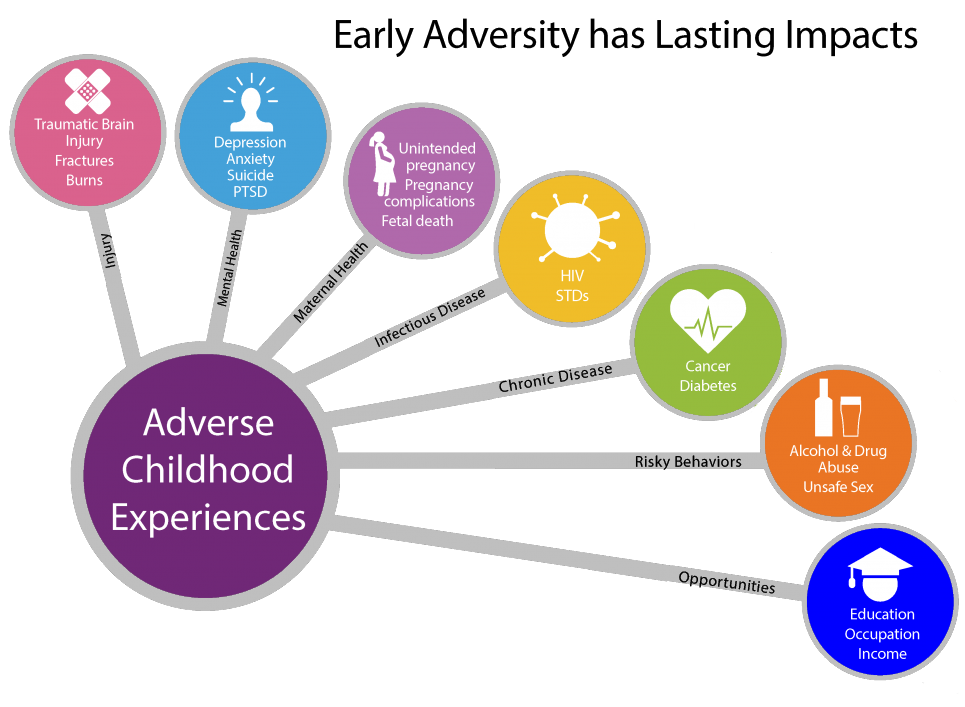
Images like this, which highlight long term physical, psychological, and society risks associated with adverse childhood experiences (ACEs) are helpful in highlighting how important it is to prevent ACEs and support people who have experienced them. An unintentional effect of such images can be making it seem like early adversity inevitably leads to these outcomes—which is not the case. It is important to consider the role of factors that protect and buffer children as well as the incredible human capacity for resilience and recovery.
Early prevention and intervention
By connecting ACEs to later physical health, this framework has captured the attention of pediatricians, who have come to view the prevalence of early adversity as a major public health crisis. Many pediatricians call for early detection and treatment by routinely screening for ACEs as part of children’s well-baby visits starting in infancy (e.g., see Dr. Nadine Burke Harris’s TED Talk). Pediatricians often screen mothers retrospectively for ACEs as well and argue for “two-generation” treatment in which they work to prevent the traumatization of young children by treating the effects of ACEs in their mothers.
This screening also provides an entry point for engaging at-risk mothers in reflection about their own childhoods and the childhoods they wish to provide for their infants. Research documenting the effects of screening is just beginning (Ford et al., 2019), but meta-analyses of interventions designed to reduce the biological impacts of childhood adversity are promising (Boparai et al., 2018). Multicomponent interventions target the reduction of ACEs by utilizing professionals to provide parenting education, mental health counseling, social service referrals, and social support. Such programs, which largely target children aged 0-5 years, have been shown to both improve parent-child relationships and reduce/reverse many neurophysiological effects in children.
Critiques of the ACEs framework.
Although the ACEs framework has been useful for practice, it has received a great deal of criticism from researchers, largely because it oversimplifies the study of early adversity. Critiques include controversy about what qualifies as an ACE, whether counting is sufficient to account for the interactions among different ACEs, and the exclusion in its calculations of any positive childhood experiences that could protect or buffer children from some or all of these neurobiological impacts (Lacey & Minnis, 2020; Sege & Browne, 2017). Many researchers also point out the problems with retrospective studies (e.g., people currently in a negative state can more easily recall negative childhood events). As a result, most researchers call for more prospective longitudinal studies that examine different kinds of adverse experiences separately. They point out that the effects of different events, like divorce versus sexual abuse, may be quite different; and that it is important to examine both the severity and chronicity of these events as well as their combination with other positive and negative experiences. As these more differentiated programs of study progress, the ACEs perspective could then provide an integrative framework within which these strands of work could be compared, contrasted, and eventually woven together.
Resilience
Just as important as research on adversity is the study of resilience. To date, such research reveals that no matter the adversity, there is always room for recuperation, gains, and workarounds to foster improvement in mental and physical functioning. For example, a recent framework called “HOPE: Health Outcomes from Positive Experiences” focuses on four broad categories of experiences that can buffer the effects of early adversity and contribute to healthy development and wellbeing: (1) nurturing, supportive relationships; (2) living, developing, playing, and learning in safe, stable, protective, and equitable environments; (3) having opportunities for constructive social engagement and connectedness; and (4) learning social and emotional competencies (Sege & Browne, 2017). In fact, the same brain characteristics that contribute to early vulnerability (i.e., malleability, meaning that the brain’s development is open to the effects of adverse experiences) also contribute to later resilience. Such “neuroplasticity” means that the developing brain can also be reshaped by subsequent positive experiences, in this case, enriching and healing social, physical, and psychological experiences. Continued exploration of the most effective components of treatment and whether they are age-graded is an important topic of study in this area.
Societal Responsibility for ACEs
As research on ACEs has become more popular, it has been subject to another major critique that also applies to all the other areas of study that focus on child maltreatment: Such work typically fails to acknowledge the role that societal factors play in creating and enabling harmful childhood experiences (e.g., Cox et al., 2018; Walsh, McCartney, Smith, & Armour, 2019). The single biggest predictor of family dysfunction and child maltreatment is the toxic stress of poverty. In the US, poverty is overrepresented in families from ethnic/racial minority backgrounds and in female-headed households, and these subgroups are subject to additional stressors and inequities based on prejudice and discrimination.
As discussed in the reading from the previous class on higher-order contexts of parenting, such hazardous conditions exert a downward pressure on people’s capacity to provide for a family and take care of children. Although most poor and minority parents accomplish these tasks successfully, it is very challenging to protect and buffer children from all of these potential risks. The developmentally dangerous conditions in which many poor children are raised can be thought of as societally sanctioned in that society has agreed that children should only receive as many of the developmental basics they need, such as food and shelter, as their families can afford. One way to significantly reduce the prevalence of ACEs would be to enact societal policies that reduce poverty. Given the expenses otherwise incurred by potential long-term behavioral and medical outcomes, such policies would not only protect and promote child health and development, they would also save a great deal of money
Center for Disease Control and Prevention: Adverse Childhood Experiences Handout [PDF]
Center for Disease Control and Prevention: Adverse Childhood Experiences website
Watch Dr. Bruce Perry talk about reducing the effects of trauma.
Additional video examples can be viewed on the CDC’s YouTube channel.
Watch Dr. Dan Siegel discuss the brain’s ability to repair after trauma.
Watch this Ted talk from pediatrician Nadine Burke Harris as she explains the impact of childhood trauma across the lifespan.
Websites
- Healthy Gender Development and Young Children The National Center of Parent, family, and Community Engagement offers these resources and tips for healthy gender development.
- CDC’s Information for Parents of Children Ages 4-11 Your child will change a lot from ages 4 to 11. At a very young age, children develop the habits and behaviors that can affect their life-long health. Use the links below to guide your child in leading a healthier life.
- The National Child Traumatic Stress Network This website provides information on early childhood trauma, which generally refers to the traumatic experiences that occur to children aged 0-6.
- This website offers queer educator Lindsay Amer’s teaching videos and resources to educate kids about gender and sexuality. bhttp://queerkidstuff.com/videos
- This study explores how typical parenting styles may not adequately capture Latinx families and underscores the importance of incorporating cultural context in any study of parenting. Domenech Rodríguez, M. M., Donovick, M. R., & Crowley, S. L. (2009). Parenting styles in a cultural context: Observations of “protective parenting” in first-generation Latinos. Family Process, 48, 195-210.
Videos
- Vygotsky’s Theory of Cognitive Development
- This video summarizes Vygotsky’s Theory of Social Development which argues that community and language play a central part in learning.
- Early Childhood Gross Motor Skills Development
- This video explains the progression of gross motor skill development in early childhood.
- Piaget – Stage 2 – Preoperational – Lack of Conservation
- This video shows a child being tested to see if she understands the law of conservation.
- The Theory of Mind Test
- Researcher Kadria Simons explains how the Theory of Mind test helps young children begin to understand other people’s thoughts and feelings.
- A Class That Turned Around Kids’ Assumptions of Gender Roles!
- When a real-life firefighter, surgeon, and fighter pilot drop in on a classroom, these kids have their assumptions about gender roles turned around.
- Like A Girl
- “In my work as a documentarian, I have witnessed the confidence crisis among girls and the negative impact of stereotypes first-hand,” said Lauren Greenfield, filmmaker and director of the video. “When the words ‘like a girl’ are used to mean something bad, it is profoundly disempowering.
- InBrief: The Science of Resilience
- This InBrief video is part two of a three-part sequence about resilience. These videos provide an overview of Supportive Relationships and Active Skill-Building Strengthen the Foundations of Resilience, a working paper from the National Scientific Council on the Developing Child.
This Ted Talk features a seasoned school teacher who discusses the importance of building strong and positive relationships with students.
This Ted Talk given by queer educator Lindsay Amer discusses why kids need to learn about gender and sexuality.
This episode of VICE takes a journey to Sweden and follows a gender non-conforming family to find out what it’s like to grow up without the gender binary.
References
American Psychological Association. (2019). Immigration. Retrieved from https://www.apa.org/advocacy/immigration
Antill, J. K., Cunningham, J. D., Cotton, S. (2003). Gender-role attitudes in middle school: In what ways do parents influence their children? Australian Journal of Psychology, 55, 148–153.
Audet, K., & Le Mare, L. (2011). Mitigating effects of the adoptive caregiving environment on inattention/overactivity in children adopted from Romanian orphanages. International Journal of Behavioral Development, 35(2), 107-115.
Baumrind, D. (1991). Parenting styles and adolescent development. In J. Brooks-Gunn, R. M. Lerner, & A. C. Petersen (Eds.), The Encyclopedia on Adolescence (pp. 746-758). New York: Garland Publishing.
Baumrind, D. (1991). The influence of parenting style on adolescent competence and substance use. Journal of Early Adolescence, 11(1), 56-95.
Baumrind, D. (2013). Authoritative parenting revisited: History and current status. In R. E. Larzelere, A. Sheffield, & A. W. Harrist (Eds.), Authoritative parenting: Synthesizing nurturance and discipline for optimal child development. Washington, DC: American Psychological Association.
Boparai, S. K. P., Au, V., Koita, K., Oh, D. L., Briner, S., Harris, N. B., & Bucci, M. (2018). Ameliorating the biological impacts of childhood adversity: a review of intervention programs. Child Abuse & Neglect, 81, 82-105.
Caldera, Y. M., Huston, A. C., & O’Brien, M. (1989). Social interactions and play patterns of parents and toddlers with feminine, masculine, and neutral toys. Child Development, 60(1), 70–76. https://doi.org/10.1111/j.1467-8624.1989.tb02696.x
Carson, D., Chowdhury, A., Perry, C., & Pati, C. (1999). Family characteristics and adolescent competence in India: Investigation of youth in southern Orissa. Journal of Youth and Adolescence, 28, 211-233
Centers for Disease Control and Prevention. (2019). About adverse childhood experiences. Retrieved from https://www.cdc.gov/violenceprevention/childabuseandneglect/acestudy/aboutace.html
Chen, L. P., Murad, M. H., Paras, M. L., Colbenson, K. M., Sattler, A. L., Goranson, E. N., … & Zirakzadeh, A. (2010, July). Sexual abuse and lifetime diagnosis of psychiatric disorders: Systematic review and meta-analysis. In Mayo Clinic Proceedings (Vol. 85, No. 7, pp. 618-629). Elsevier.
Chang, L., Schwartz, D., Dodge, K. A., & McBride-Chang, C. (2003). Harsh parenting in relation to child emotion regulation and aggression. Journal of Family Psychology, 17(4), 598-606. doi:http://dx.doi.org.proxy.lib.pdx.edu/10.1037/0893-3200.17.4.598
Chao, R. K. (1994). Beyond parental control and authoritarian parenting style: Understanding Chinese parenting through the cultural notion of training. Child Development, 65, 1111-1119.
Colman, R. A., Hardy, S. A., Albert, M., Raffaelli, M., & Crockett, L. (2006). Early predictors of self‐regulation in middle childhood. Infant and Child Development, 15(4), 421-437.
Cooley, C.H. (1964) Human nature and the social order. Schocken, New York.
Cox, K. S., Sullivan, C. G., Olshansky, E., Czubaruk, K., Lacey, B., Scott, L., & Van Dijk, J. W. (2018). Critical conversation: Toxic stress in children living in poverty. Nursing Outlook, 66(2), 204-209.
Curenton, S. M., Iruka, I. U., & Harnett, N. G. (2023). The Brain Architects Podcast: Understanding racism’s impact on child development. Center on the Developing Child at Harvard University. https://developingchild.harvard.edu/brain-architects-podcast-understanding-racisms-impact-on-child-development/
Darling, N. (1999). Parenting style and its correlates. ERIC digest. Retrieved from https://www.ericdigests.org/1999-4/parenting.htm
Dmitrieva, J., Chen, C., Greenberger, E., & Gil-Rivas, V. (2004). Family relationships and adolescent psychosocial outcomes: Converging findings from Eastern and Western cultures. Journal of Research on Adolescence, 14, 425-447.
Dougherty, D.M., Marsh, D.M., Mathias, C.W., & Swann, A.C. (2005). The conceptualization of impulsivity: Bipolar disorder and substance abuse. Psychiatric Times, 22(8), 32-35.
Egan, S., Perry, D., G. & Dannemiller, J.L. (2001). Gender Identity: A multidimensional analysis with implications for psychosocial adjustment. Developmental Psychology, 37(4), 451–463.
Eisenberg, N., Sadovsky, A., & Spinrad, T. L. (2005). Associations of emotion‐related regulation with language skills, emotion knowledge, and academic outcomes. New directions for child and adolescent development, 2005(109), 109-118.
Erikson, E. (1982). The life cycle completed. NY: Norton & Company.
Fagot, B. I., & Leinbach, M. D. (1989). The young child’s gender schema: Environmental input, internal organization. Child Development, 60(3), 663–672
Fay-Stammbach, T., Hawes, D. J., & Meredith, P. (2014). Parenting influences on executive function in early childhood: A review. Child Development Perspectives, 8(4), 258-264.
Felitti, V. J., Anda, R.F., Nordenberg, D., Williamson, D. F., Spitz, A., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245-258. doi:10.1016/S0749-3797(98)00017-8
Ford, K., Hughes, K., Hardcastle, K., Di Lemma, L. C., Davies, A. R., Edwards, S., & Bellis, M. A. (2019). The evidence base for routine enquiry into adverse childhood experiences: A scoping review. Child Abuse & Neglect, 91, 131-146.
Halim, M. L., & Ruble, D. (2010). Gender identity and stereotyping in early and middle childhood. In Handbook of Gender Research in Psychology (pp. 495–525). Springer: New York.
Harvard University. (2019). Center on the developing child: Toxic stress. Retrieved from https://developingchild.harvard.edu/science/key-concepts/toxic-stress/
Harvard Center on the Developing Child. (2023). Early childhood adversity, toxic stress, and the impacts of racism on the foundations of health. Harvard University. https://scholar.harvard.edu/files/davidrwilliams/files/early_childhood_adversity_toxic_stress_and_the_impacts_of_racism_on_the_foundations_of_health.pdf
Killen, M., & Stangor, C. (2001). Children’s social reasoning about inclusion and exclusion in gender and race peer group contexts. Child Development, 72(1), 174–186
Kimmel, M. S. (2008). The gendered society (3rd ed.). Oxford: Oxford University Press.
Kochanska, G. (2002). Mutually responsive orientation between mothers and their young children: A context for the early development of conscience. Current Directions in Psychological Science, 11(6), 191-195.
Kuhn, D., Nash, S. C., & Brucken, L. (1978). Sex role concepts of two-and three-year-olds. Child Development, 49(2), 445–451
Lacey, R. E., & Minnis, H. (2020). Practitioner Review: Twenty years of research with adverse childhood experience scores–Advantages, disadvantages and applications to practice. Journal of Child Psychology and Psychiatry, 61(2), 116-130.
Langlois, J. H., & Downs, A. C. (1980). Mothers, fathers, and peers as socialization agents of sex-typed play behaviors in young children. Child Development, 51(4), 1237–1247.
Maccoby, E., & Jacklin, C. (1987). Gender segregation in childhood. Advances in Child Development and Behavior, 20, 239-287.
Martin, C. L., Ruble, D. N., & Szkrybalo, J. (2004). Recognizing the centrality of gender identity and stereotype knowledge in gender development and moving toward theoretical integration: reply to Bandura and Bussey. Psychological Bulletin, 130(5), 702–710.
Mayseless, O., Scharf, M., & Sholt, M. (2003). From authoritative parenting practices to an authoritarian context: Exploring the person-environment fit. Journal of Research on Adolescence, 17, 23-50.
McLean Hospital. (2023, February 1). Racial disparities in childhood adversity linked to brain structural differences in U.S. children. ScienceDaily. https://www.sciencedaily.com/releases/2023/02/230201084347.htm
Mead, G. H. (1967). Mind, self, and society: from the standpoint of a social behaviorist. USA: University of Chicago
Merrick, M. T., Ford, D. C., Ports, K. A., & Guinn, A. S. (2018). Prevalence of adverse childhood experiences from the 2011- 2014 Behavioral Risk Factor Surveillance System in 23 States. Early JAMA Pediatrics, 172(11), 1038-1044.
Middlebrooks, J. S., & Audage, N. C. (2008). The effects of childhood stress on health across the lifespan. (United States, Center for Disease Control, National Center for Injury Prevention and Control). Atlanta, GA.
Miller, C. F., Lurye, L. E., Zosuls, K. M., & Ruble, D. N. (2009). Accessibility of gender stereotype domains: Developmental and gender differences in children. Sex Roles, 60(11-12), 870–881
Mischel, W., Ayduk, O., Berman, M. G., Casey, B. J., Gotlib, I. H., Jonides, J., & … Shoda, Y. (2011). ‘Willpower’ over the life span: Decomposing self-regulation. Social Cognitive & Affective Neuroscience, 6(2), 252-256. doi:10.1093/scan/nsq081
Mischel, W., Ebbesen, E. B., & Zeiss, A. R. (1972). Cognitive and attentional mechanisms in delay of gratification. Journal of Personality and Social Psychology, 21, 204–218.
Morris, A. S., Silk, J. S., Morris, M. D., Steinberg, L., Aucoin, K. J., & Keyes, A. W. (2011). The influence of mother–child emotion regulation strategies on children’s expression of anger and sadness. Developmental psychology, 47(1), 213.
Petruccelli, K., Davis, J., & Berman, T. (2019). Adverse childhood experiences and associated health outcomes: A systematic review and meta-analysis. Child Abuse & Neglect, 97, 104127.
Pilgrim, C., Luo, Q., Urberg, K.A., & Fang, X. (1999). Influence of peers, parents, and individual characteristics on adolescent drug use in two cultures. Merril-Palmer Quarterly, 45, 85-107.
Punamaki, R., Qouta, S., & Sarraj, E. (1997). Models of traumatic experiences and children’s psychological adjustment: The roles of perceived parenting and the children’s own resources and activity. Child Development, 68, 718-728.
Raikes, H. A., Robinson, J. L., Bradley, R. H., Raikes, H. H., & Ayoub, C. C. (2007). Developmental trends in self‐regulation among low‐income toddlers. Social Development, 16(1), 128-149.
Rothbart, M. K., Sheese, B. E., Rueda, M. R., & Posner, M. I. (2011). Developing mechanisms of self-regulation in early life. Emotion review, 3(2), 207-213.
Sadker, M., & Sadker, D. M. (1994). Failing at fairness: How America’s schools cheat girls. New York: C. Scribner’s Sons.
Sege, R. D., & Browne, C. H. (2017). Responding to ACEs with HOPE: Health outcomes from positive experiences. Academic Pediatrics, 17(7), S79-S85.
Sperber, J. F., Vandell, D. L., Duncan, G. J., Watts, T. W. (2024). Delay of gratification and adult outcomes: The Marshmallow Test does not reliably predict adult functioning. Child Development, 00, (1-15) https://doi.org/10.1111/cdev.14129″>https://doi.org/10.1111/cdev.14129
Steinberg, L. (2001). We know some things: Adolescent-parent relationships in retrospect and prospect. Journal of Research on Adolescence, 11, 1-19.
Strauss, E. (April 2018). “Why girls can be boyish but boys can’t be girlish”. CNN. https://www.cnn.com/2018/04/12/health/boys-girls-gender-norms-parenting-strauss/index.html. ↵
Thompson, R. A. (2012). Whither the preconventional child? Toward a life‐span moral development theory. Child development perspectives, 6(4), 423-429.
Thompson, R. A., & Goodvin, R. (2007). Taming the tempest in the teapot. Socioemotional development in the toddler years: Transitions and transformations, 320-341.
Trautner, H. M., Ruble, D. N., Cyphers, L., Kirsten, B., Behrendt, R., & Hartmann, P. (2005). Rigidity and flexibility of gender stereotypes in childhood: developmental or differential? Infant and Child Development, 14(4), 365–381.
Traverso, L., Viterbori, P., & Usai, M. C. (2015). Improving executive function in childhood: Evaluation of a training intervention for 5-year-old children. Frontiers in Psychology, 6, 1-14. doi:10.3389/fpsyg.2015.00525
Walsh, D., McCartney, G., Smith, M., & Armour, G. (2019). Relationship between childhood socioeconomic position and adverse childhood experiences (ACEs): A systematic review. Journal Epidemiol Community Health, 73(12), 1087-1093.
Watts, T. W., Duncan, G. J., & Quan, H. (2018). Revisiting the Marshmallow Test: A Conceptual Replication Investigating Links Between Early Delay of Gratification and Later Outcomes. Psychological science, 29(7), 1159–1177. https://doi.org/10.1177/0956797618761661
Weinraub, M., Clemens, L. P., Sockloff, A., Ethridge, T., Gracely, E., & Myers, B. (1984). The development of sex role stereotypes in the third year: Relationships to gender labeling, gender identity, sex-typed toy preference, and family characteristics. Child Development, 55(4), 1493–1503.
Weiss, L. H., & Schwarz, J. C. (1996). The relationship between parenting types and older adolescents’ personality, academic achievement, adjustment, and substance use. Child Development, 67(5), 2101-2114. EJ 539 840.
World Health Organization (2011). Gender and genetics: Sex selection and the law. http://www.who.int/genomics/gender/en/index4.html
Witt, S. (1997). Parental Influence on Children’s Socialization to Gender Roles. Adolescence, 32(126), 253–259.
Zosuls, K. M., Miller, C. F., Ruble, D. N., Martin, C. L., & Fabes, R. A. (2011). Gender Development Research in Sex Roles: Historical Trends and Future Directions. Sex Roles, 64(1112)
Attributions
“Lifespan Development: A Psychological Perspective, Second Edition” by Martha Lally and Suzanne Valentine-French is licensed under a CC-BY-NC-SA-3.0
Lifespan Development by Lumen Learning is licensed under a Creative Commons Attribution 4.0 International License
Additional materials (Behavioral and Emotional Regulation) by Ellen Skinner & Eli Labinger, Portland State University is licensed under a CC-BY-NC-SA-4.0
Child Growth and Development by College of the Canyons, Jennifer Paris, Antoinette Ricardo, and Dawn Rymond and is used under a CC BY 4.0 international license
Introduction to Sociology 2e by Rice University is licensed under a CC BY-NC-SA 4.0 License. / modified and adapted by Ellen Skinner & Heather Brule, Portland State University
Additional written material by Ellen Skinner, Portland State University is licensed under CC BY-NC-SA 4.0
Human Growth and Development by Ryan Newton is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License,
Individual and Family Development, Health, and Well-being by Diana Lang, Nick Cone; Laura Overstreet, Stephanie Loalada; Suzanne Valentine-French, Martha Lally; Julie Lazzara, and Jamie Skow is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License,
Human Development by Human Development Teaching & Learning Group under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License,
Support for Baumrind’s Authoritative Parenting is taken from The Family by Joel A Muraco, licensed CC BY NC SA.
Baumrind’s Parenting Styles is an adaptation of Child, Family, and Community (Chapter 6: A Closer Look at Parenting) by Laff & Ruiz (2019), licensed CC BY 4.0 and Social and Personality Development in Childhood by Ross Thompson, licensed CC BY NC SA.
- Table 1 Source: Development through the Lifespan by Alisa Beyer and Julie Lazzara, licensed CC BY NC SA, ↵

.jpg){kind=link}
{kind=link}