Section 11: Late Adulthood
11.4 Psychosocial Development in Late Adulthood
What are psychosocial changes in late adulthood?

Our ideas about aging and what it means to be over 50, over 60, or even over 90 seem to be stuck somewhere back in the middle of the 20th century. We still consider 65 to be the standard retirement age, and we expect everyone to start slowing down and moving aside for the next generation as their age passes the half-century mark. In this section, we explore psychosocial developmental theories, including Erik Erikson’s theory on psychosocial development in late adulthood, and we look at aging as it relates to work, retirement, and leisure activities for older adults. We’ll also examine ways in which people are productive in late adulthood.
Learning Objectives
- Describe psychosocial development in late adulthood
- Describe the different psychosocial theories of aging.
- Describe theories related to late adulthood, including Erikson’s psychosocial stage of integrity vs. despair,.
- Describe examples of productivity in late adulthood
- Describe attitudes about aging
- Examine family relationships during late adulthood (grandparenting, marriage, divorce, widowhood, traditional and non-traditional roles; co-habitation, LGBTQ+)
Psychosocial Development in Late Adulthood
Erikson’s Theory
| Table 1. Erikson’s Psychosocial Stages of Development | |||
|---|---|---|---|
| Stage | Age (years) | Developmental Task | Description |
| 1 | 0–1 | Trust vs. mistrust | Trust (or mistrust) that basic needs, such as nourishment and affection, will be met |
| 2 | 1–3 | Autonomy vs. shame/doubt | Develop a sense of independence in many tasks |
| 3 | 3–6 | Initiative vs. guilt | Take initiative on some activities—may develop guilt when unsuccessful or boundaries overstepped |
| 4 | 7–11 | Industry vs. inferiority | Develop self-confidence in abilities when competent or a sense of inferiority when not |
| 5 | 12–18 | Identity vs. Confusion | Experiment with and develop identity and roles |
| 6 | 19–29 | Intimacy vs. isolation | Establish intimacy and relationships with others |
| 7 | 30–64 | Generativity vs. stagnation | Contribute to society and be part of a family |
| 8 | 65– | Integrity vs. despair | Assess and make sense of life and meaning of contributions |
Erikson: Integrity vs. Despair
Like all psychosocial tasks, this one has two potential resolutions: Integrity, or a sense of self-acceptance, contentment with life and imminent death, versus Despair, or a lack of fulfillment or peace and the inability to come to terms with life, aging, and approaching death.
As people age and enter their retirement years, the pace of life and productivity tend to slow down, granting them time for reflection upon their lives. They may ask the existential question, “Is it okay to have been me?” If someone sees themselves as having lived a successful life, they may see it as one filled with productivity or, according to Erik Erikson, integrity.
Erikson framed the last part of the lifespan with the developmental task of Integrity versus Despair. In terms of psychosocial development, the tasks of adulthood were about becoming the self that you want to become (i.e., Identity) and creating the life you want to live, including establishing or maintaining the close interpersonal relationships that will be crucial to your physical and psychological health and well -being (i.e., Intimacy). The value of that life project is negotiated during middle adulthood in the search for meaning and a purpose larger than yourself that will contribute to your legacy (i.e., Generativity).
So in old age, this final task basically comes down to whether you have built a life and constructed a self that is sufficient to withstand the disintegration of your physical body, the death of many of those you love, and eventually and inevitably, strong enough to face your own impending death with dignity and grace.
Here, integrity is said to consist of the ability to look back on one’s life with a feeling of satisfaction, peace, and gratitude for all that has been given and received. Erikson (1959/1980) notes in this regard:
“The possessor of integrity is ready to defend the dignity of his own lifestyle against all physical and economic treats. For he knows that an individual life is the accidental coincidence of but one life cycle within but one segment of history; and that for him all human integrity stands and falls with the one style of integrity of which he partakes.” (p. 104)
Thus, persons derive a sense of meaning (i.e., integrity) through a careful review of how their lives have been lived (Krause, 2012). Ideally, however, integrity does not stop here but rather continues to evolve into the virtue of wisdom. According to Erikson, this is the goal during this stage of life.
Development during elderhood, as during all developmental periods, is a bio-psycho-social process that takes place in specific societal and historical contexts. But this task, at the end of life, offers us the prospect of lifting off of those geographical, societal, and temporal limitations. We have the potential to transcend them, to establish a sense of wholeness and acceptance by getting in touch with our universal connection to humanity, past, present, and future. Like birth, death is a journey that every single one of us will take.
If a person sees their life as unproductive or feels that they did not accomplish their life goals, they may become dissatisfied with life and develop what Erikson calls despair, often leading to depression and hopelessness. This stage can occur out of the sequence when an individual feels they are near the end of their life (such as when receiving a terminal disease diagnosis).

Erikson’s Ninth Stage
Erikson collaborated with his wife, Joan, throughout much of his work on psychosocial development. In Erikson’s older years, they re-examined the eight stages and generated additional ideas about how development evolves during a person’s 80s and 90s. After Erik Erikson passed away in 1994, Joan published a chapter on the ninth stage of development, in which she proposed (from her own experiences and Erikson’s notes) that older adults revisit the previous eight stages and deal with the previous conflicts in new ways, as they cope with the physical and social changes of growing old.
In the first eight stages, all of the conflicts are presented in a syntonic-dystonic manner, meaning that the first term listed in the conflict is the positive, sought-after achievement, and the second term is the less desirable goal (i.e., trust is more desirable than mistrust, and integrity is more desirable than despair) (Perry et al., 2015).
During the ninth stage, the Eriksons argue that the dystonic, or less desirable outcome, comes to take precedence again. For example, an older adult may become mistrustful (trust vs. mistrust), feel more guilt about not having the abilities to do what they once did (initiative vs. guilt), feel less competent compared with others (industry vs. inferiority), lose a sense of identity as they become dependent on others (identity vs. role confusion), become increasingly isolated (intimacy vs. isolation), and feel that they have less to offer society (generativity vs. stagnation) (Gusky, 2012). The Eriksons found that those who successfully come to terms with these changes and adjustments in later life make headway towards gerotranscendence, a term coined by gerontologist Lars Tornstam to represent a greater awareness of one’s own life and connection to the universe, increased ties to the past, and a positive, transcendent, perspective about life.
Theories of Aging: Activity and Disengagement
Activity Theory. Developed by Havighurst and Albrecht in 1953, activity theory addresses the issue of how persons can best adjust to the changing circumstances of old age–e.g., retirement, illness, loss of friends and loved ones through death, and so on. In addressing this issue, they recommend that older adults involve themselves in voluntary and leisure organizations, child care, and other forms of social interaction. Activity theory thus strongly supports the avoidance of a sedentary lifestyle and considers it essential to health and happiness that the older person remains active physically and socially. In other words, the more active older adults are, the more stable and positive their self-concept will be, which will then lead to greater life satisfaction and higher morale (Havighurst & Albrecht, 1953). Activity theory suggests that many people are barred from meaningful experiences as they age, but older adults who continue to find ways to remain active can work toward replacing lost opportunities with new ones (Nilsson et al., 2015).
Disengagement theory, developed by Cumming and Henry in the 1950s (Cumming & Henry, 1961), in contrast to activity theory, emphasizes that older adults should not be discouraged from following their inclination towards solitude and greater inactivity. While not completely discounting the importance of exercise and social activity for the upkeep of physical health and personal well-being, disengagement theory is opposed to artificially keeping the older person so busy with external activities that they have no time for contemplation and reflection (Cumming & Henry, 1961).
In other words, disengagement theory posits that older adults in all societies undergo a process of adjustment that involves leaving former public and professional roles and narrowing their social horizons to a smaller circle of family and friends. This process enables the older person to die more peacefully, without the stress and distractions that come with a more socially involved life. The theory suggests that during late adulthood, the individual and society mutually withdraw. Older people become more isolated from others and less concerned or involved with life in general. This once-popular theory is now criticized as being ageist and used in order to justify treating older adults as second-class citizens (Nilsson et al., 2015).
Continuity theory suggests as people age, they continue to view the self in much the same way as they did when they were younger. An older person’s approach to problems, goals, and situations is much the same as it was when they were younger. They are the same individuals, but simply in older bodies. Consequently, older adults continue to maintain their identity even as they give up previous roles. For example, a retired Coast Guard commander attends reunions with shipmates, stays interested in new technology for home use, is meticulous in the jobs he does for friends or at church, and displays mementos from his experiences on the ship. He is able to maintain a sense of self as a result. People do not give up who they are as they age. Hopefully, they are able to share these aspects of their identity with others throughout life. Focusing on what a person can do and pursuing those interests and activities is one way to optimize and maintain self-identity.
Generativity in Late Adulthood
People in late adulthood continue to be productive in many ways. These include work, education, volunteering, family life, and intimate relationships. Older adults also experience generativity (recall Erikson’s previous stage of generativity vs. stagnation) through voting, forming and helping social institutions like community centers, churches and schools. Thinking of the issue of legacy, psychoanalyst Erik Erikson wrote “I am what survives me” (Havey, 2015).

Productivity in Work. Some older people continue to be productive in work. Mandatory retirement is now illegal in the United States. However, many do choose retirement by age 65. Most people leave work by choice, and the primary factors that influence decisions about when to retire are health status, finances, and satisfaction at work. Those who do leave by choice adjust to retirement more easily. Chances are, they have prepared for a smoother transition by gradually giving more attention to an avocation or interest as they approach retirement. And they are more likely to be financially ready to retire. Those who must leave abruptly for health reasons or because of layoffs or downsizing have a more difficult time adjusting to their new circumstances. Men, especially, can find unexpected retirement difficult.
Women may feel less of an identity loss after retirement because much of their identity may have come from family roles as well. At the same time, however, women tend to have poorer retirement funds accumulated from work, and if they take their retirement funds in a lump sum (be that from their own or from a deceased husband’s funds), they are more at risk of outliving those funds. Because they will, on average, live longer, women need better financial planning in retirement. Sixteen percent of adults over 65 were in the labor force in 2008 (U. S. Census Bureau 2011). Globally, 6.2% are in the labor force and this number is expected to reach 10.1 million by 2016. Many adults 65 and older continue to work either full-time or part-time, either for income or pleasure, or both. In 2003, 39% of full-time workers over 55 were women over the age of 70; 53% were men over 70. This increase in the number of older adults is likely to mean that more will continue to be part of the workforce in years to come (He et al., 2005).
Sixteen percent of adults over 65 were in the labor force in 2008 (Census Bureau, 2011). Globally, 6.2 percent are in the labor force, and this number is expected to reach 10.1 million by 2016. Many adults 65 and older continue to work either full-time or part-time, either for income or pleasure, or both. In 2003, 39 percent of full-time workers over 55 were women over the age of 70; 53 percent were men over 70. This increase in the number of older adults is likely to mean that more will continue to be part of the workforce in years to come (He et al., 2005).
Volunteering: Face-to-face and Virtually. About 40% of older adults are involved in some type of structured, face-to-face volunteer work. Many older adults, about 60%, engage in a sort of informal type of volunteerism, helping out neighbors or friends rather than working in an organization (Berger, 2005). They may help a friend by taking them somewhere or shopping for them, etc. Some do participate in organized volunteer programs, but interestingly enough, those who do tend to work part-time as well. Those who retire and do not work are less likely to feel that they have a contribution to make. (It’s as if when one gets used to staying at home, one’s confidence to go out into the world diminishes.) And those who have recently retired are more likely to volunteer than those over 75 years of age.
Hooyman and Kiyak (2011) found that religious organizations are the primary settings for encouraging and providing volunteer opportunities. Hospitals and environmental groups also provide volunteer opportunities for older adults.
New opportunities exist for older adults to serve as virtual volunteers by dialoguing online with others from around the world and sharing their support, interests, and expertise. According to an article from the American Association of Retired Persons (AARP), virtual volunteerism has increased from 3,000 participants in 1998 to over 40,000 in 2005. These volunteer opportunities range from helping teens with their writing to communicating with ‘neighbors’ in villages in developing countries. Virtual volunteering is available to those who cannot engage in face-to-face interactions and opens up a new world of possibilities and ways to connect, maintain identity, and be productive (Uscher, 2006).
Volunteering aids older adults as much as it does the community at large. Older adults who volunteer experience more social contact, which has been linked to higher rates of life satisfaction and lower rates of depression and anxiety (Pilkington, Windsor, & Crisp, 2012). Longitudinal research also finds a strong link between health in later adulthood and volunteering (Kahana, et al., 2013). Lee and colleagues found that even among the oldest-old, the death rate of those who volunteer is half that of non-volunteers (Lee et al., 2011). However, older adults who volunteer may already be healthier, which is why they can volunteer compared to their less healthy age mates.
Education. Twenty percent of people over 65 have a bachelor’s or higher degree. And over 7 million people over 65 take adult education courses (Census Bureau, 2011). Lifelong learning through continuing education programs on college campuses or programs known as “Elderhostels,” which allow older adults to travel abroad, live on campus, and study, provide enriching experiences. Academic courses, as well as practical skills such as computer classes, foreign languages, budgeting, and holistic medicines, are among the courses offered. Older adults who have higher levels of education are more likely to take continuing education. However, offering more educational experiences to a diverse group of older adults, including those who are institutionalized in nursing homes, can enhance the quality of life.
Religious Activities. People tend to become more involved in prayer and religious activities as they age. This provides a social network and a belief system that can combat the fear of death. Religious activities also provide a focus for volunteerism and other activities. For example, one elderly woman prides herself on knitting prayer shawls that are given to those who are sick. Another serves on the altar guild and is responsible for keeping robes and linens clean and ready for communion.
Political Activism. The elderly are very politically active. They have high voter turnout rates and engage in letter writing to Congress on issues that affect them and a wide range of domestic and foreign concerns. In the past three presidential elections, over 70 percent of people 65 and older showed up at the polls to vote (Census Bureau, 2011).
Try It
Attitudes about Aging
Stereotypes about people in late adulthood lead many to assume that aging automatically brings poor health and mental decline (Figure 4). These stereotypes are reflected in everyday conversations, the media, and even in greeting cards.[1] The following examples serve to illustrate:
- Grandpa, fishing pole in one hand, pipe in the other, sits on the ground and completes a story being told to his grandson with “. . . and that, Jimmy, is the tale of my very first colonoscopy.” The message inside the card reads, “Welcome to the gross personal story years.” (Shoebox, A Division of Hallmark Cards.)
- An older woman in a barbershop cuts the hair of an older, dozing man. “So, what do you say today, Earl?” she asks. The inside message reads, “Welcome to the age where pretty much any place is a good place for a nap.” (Shoebox, A Division of Hallmark Cards.)
- A crotchety old man with wire glasses, a crumpled hat, and a bow tie grimaces, and the card reads, “Another year older? You’re at the age where you should start eatin’ right, exercisin’, and takin’ vitamins . . .” The inside reads, “Of course, you’re also at the age where you can ignore advice by actin like you can’t hear it.” (Hallmark Cards, Inc.)
Of course, these cards are made because they are popular. Age is not revered in the United States, and so laughing about getting older is one way to get relief. The attitudes above are examples of ageism and prejudice based on age. Ageism is prejudice and discrimination that is directed at older people. The term ageism was first used in 1969, and according to Nelson (2016), Ageism remains one of the most institutionalized forms of prejudice today. Nelson (2016) reviewed the research on ageism and concluded that when older individuals believed their culture’s negative stereotypes about those who are old, their memory and cognitive skills declined. In contrast, older individuals in cultures such as China who held more positive views on aging did not demonstrate cognitive deficits. This view suggests that older people are less in command of their mental faculties. Older people are viewed more negatively than younger people on a variety of traits, particularly those relating to general competence and attractiveness. Stereotypes such as these can lead to a self-fulfilling prophecy in which beliefs about one’s ability result in actions that make it come true.

Ageism is a modern and predominately Western cultural phenomenon—in the American colonial period, long life was an indication of virtue, and Asian and Native American societies view older people as wise, storehouses of information about the past, and deserving of respect. Many preindustrial societies observed gerontocracy, a type of social structure wherein the power is held by a society’s oldest members. In some countries today, the elderly still have influence and power, and their vast knowledge is respected, but this reverence has decreased in many places due to social factors. A positive, optimistic outlook about aging and the impact one can have on improving health is essential to health and longevity. Removing societal stereotypes about aging and helping older adults reject those notions of aging is another way to promote health in older populations.
In addition to ageism, racism is yet another concern for minority populations as they age. The number of black Americans above the age of 65 is projected to grow from around 4 million now to 12 million by 2060. Racism towards black people and other minoritized groups throughout their lifetime results in many older minoritized people having fewer resources, more chronic health conditions, and significant health disparities when compared to older white Americans. Racism towards older adults from diverse backgrounds has resulted in them having limited access to community resources such as grocery stores, housing, health care providers, and transportation (American Psychological Association, n.d.)
Elderly Abuse
Nursing homes have been publicized as places where older adults are at risk of abuse. Abuse and neglect of nursing home residents is more often found in facilities that are run down and understaffed. However, older adults are more frequently abused by family members. The most commonly reported types of abuse are financial abuse and neglect. Victims are usually very frail and impaired, and perpetrators are usually dependent on the victims for support. Prosecuting a family member who has financially abused a parent is very difficult. The victim may be reluctant to press charges, and the court dockets are often very full, resulting in long waits before a case is heard. “Granny dumping,” or the practice of family members abandoning older family members with severe disabilities in emergency rooms, is a growing problem; an estimated 100,000 and 200,000 are dumped each year (Berk, 2007).
This clip from the Big Think examines some of the negative prejudices about the elderly.
You can watch another video from Ashton Applewhite in this TED talk “Let’s End Ageism.”
Try It
Relationships in Late Adulthood
During late adulthood, many people find that their relationships with their adult children, siblings, spouses, or life partners change. Roles may also change, as many are grandparents or great-grandparents, caregivers to even older parents or spouses, or receivers of care in a nursing home or other care facility.[
Relationship with Adult Children. Many older adults provide financial assistance and/or housing to adult children. At this point in history, more support is going from the older parent to the younger adult children than in the other direction (Fingerman & Birditt, 2011). In addition to providing for their own children, many elders are raising their grandchildren. Consistent with the socioemotional selectivity theory, older adults seek and are helped by their adult children’s emotional support (Lang & Schütze, 2002).
Lang and Schütze, as part of the Berlin Aging Study (BASE), surveyed adult children (mean age 54) and their aging parents (mean age 84). They found that the adult children of older parents who provided emotional support, such as showing tenderness toward their parent and cheering the parent up when he or she was sad, tended to report greater life satisfaction. In contrast, older adults whose children provided informational support, such as providing advice to the parent, reported less life satisfaction. They found that older adults wanted their relationship with their children to be more emotionally meaningful, but they did not want their children telling them what to do. Daughters and adult children who were younger tended to provide such support more than sons and adult children who were older. Lang and Schütze also found that adult children who were more autonomous rather than emotionally dependent on their parents had more emotionally meaningful relationships with their parents from both the parent’s and adult children’s points of view.
Friendships. Friendships are not formed in order to enhance status or careers and may be based purely on a sense of connection or the enjoyment of being together. Most elderly people have at least one close friend. These friends may provide emotional as well as physical support. Being able to talk with friends and rely on others is very important during this stage of life. Bookwala et al. (2014) found that the availability of a friend played a significant role in protecting women’s health from the impact of widowhood. Specifically, those who became widowed and had a friend as a confidante reported significantly lower somatic depressive symptoms, better self-rated health, and fewer sick days in bed than those who reported not having a friend as a confidante. In contrast, having a family member as a confidante did not provide health protection for those recently widowed.

Grandparenting. It has become increasingly common for grandparents to live with and raise their grandchildren or to move back in with adult children in their later years. According to the U.S. Census Bureau, 2.7 million grandparents raised their grandchildren in 2009. The dramatic increase in grandparent-headed households has been attributed to many factors, including parental substance abuse.
Grandparenting typically begins in midlife rather than late adulthood, but because people are living longer, they can anticipate being grandparents for longer periods of time. Cherlin and Furstenberg (1986) describe three styles of grandparents:
1. Remote Grandparents: These grandparents rarely see their grandchildren. Usually they live far away from the grandchildren, but may also have a distant relationship. Contact is typically made on special occasions such as holidays or birthdays. Thirty percent of the grandparents studied by Cherlin and Furstenberg were remote.[2]
2. Companionate Grandparents: Fifty-five percent of grandparents studied were described as companionate. These grandparents do things with the grandchild but have little authority or control over them. They prefer to spend time with them without interfering in parenting. They are more like friends to their grandchildren.
3. Involved Grandparents: Fifteen percent of grandparents were described as involved. These grandparents take a very active role in their grandchild’s life. The grandchildren might even live with their grandparents. The involved grandparent is one who has frequent contact with and authority over the grandchild.
Grandparents raising Grandchildren. According to the 2014 American Community Survey (2014a), over 5.5 million children under the age of 18 were living in families headed by a grandparent, more than a half-million increase from 2010. While most grandparents raising grandchildren are between the ages of 55 and 64, approximately 25% of grandparents raising their grandchildren are 65 and older (Office on Women’s Health, 2010a).
For many grandparents, parenting a second time can be harder. Older adults have far less energy, and often, the reason why they are now acting as parents to their grandchildren is because of traumatic events. A survey by AARP (Goyer, 2010) found that grandparents were raising their grandchildren because the parents had problems with drugs and alcohol, had a mental illness, were incarcerated, had divorced, had a chronic illness, were homeless, had neglected or abused the child, were deployed in the military, or had died. While most grandparents state they gain great joy from raising their grandchildren, they also face greater financial, health, education, and housing challenges that often derail their retirement plans than do grandparents who do not have primary responsibility for raising their grandchildren.
Marriage and Divorce
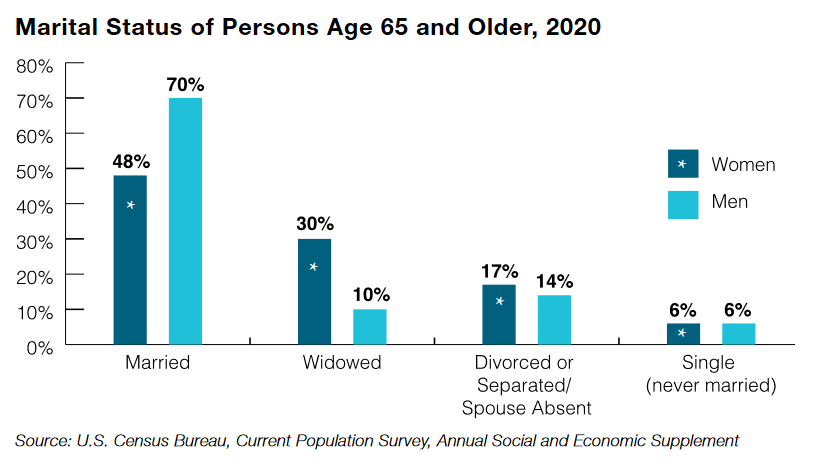
Most males and females aged 65 and older had been married at some point in their lives. According to the U.S. Census Bureau, 2016 American Community Survey, among the population 65 and older, males were significantly more likely to be married (70 percent) compared with females (44 percent) in the same age group. Even in the oldest age group, 85 and older, 54 percent of males were still married compared with 15 percent of females (Roberts & Stella, 2016).

Twelve percent of older men and 15% percent of older women have been divorced, and about 6 percent of older adults have never married (Roberts & Stella, 2016). Many married couples feel their marriage has improved with time, and the emotional intensity and level of conflict that might have been experienced earlier has declined. This is not to say that bad marriages become good ones over the years, but that those marriages that were very conflict-ridden may no longer be together and that many of the disagreements couples might have had earlier in their marriages may no longer be concerns. Children have grown, and the division of labor in the home has probably been established. Men tend to report being satisfied with marriage more than women. Women are more likely to complain about caring for a spouse who is ill or accommodating a retired husband and planning activities. Older couples continue to engage in sexual activity but with less focus on intercourse and more on cuddling, caressing, and oral sex. (Carroll, 2007).
Divorce after long-term marriage does occur, but is not as common as earlier divorces, despite rising divorce rates for those above age 65. Older adults who have been divorced since midlife tend to have settled into comfortable lives and, if they have raised children, to be proud of their accomplishments as single parents. Remarriage is also on the rise for older adults; in 2014, 50% of adults ages 65 and older had remarried, up from 34% in 1960. Men are also more likely to remarry than women (Livingston, 2014).
Dating. Due to changing social norms and shifting cohort demographics, it has become more common for single older adults to be involved in dating and romantic relationships (Alterovitz & Mendelsohn, 2011). An analysis of widows and widowers ages 65 and older found that 18 months after the death of a spouse, 37% of men and 15% of women were interested in dating (Carr, 2004a). Unfortunately, opportunities to develop close relationships often diminish in later life as social networks decrease because of retirement, relocation, and the death of friends and loved ones (de Vries, 1996). Consequently, older adults, much like those younger, are increasing their social networks using technologies, including e-mail, chat rooms, and online dating sites (Fox, 2004; Wright & Query, 2004; Papernow, 2018).
Interestingly, older men and women parallel online dating information as those younger. Alterovitz and Mendelsohn (2011) analyzed 600 Internet personal ads from different age groups, and across the lifespan, men sought physical attractiveness and offered status-related information more than women. With advanced age, men desired women increasingly younger than themselves, whereas women desired older men until ages 75 and over when they sought men younger than themselves. Research has previously shown that older women in romantic relationships are not interested in becoming a caregiver or becoming widowed for a second time (Carr, 2004a).
Additionally, older men are more eager to repartner than are older women (Davidson, 2001; Erber & Szuchman, 2015). Concerns expressed by older women included not wanting to lose their autonomy, care for a potentially ill partner, or merge their finances with someone (Watson & Stelle, 2011). Older dating adults also need to know about threats to sexual health, including being at risk for sexually transmitted diseases, including chlamydia, genital herpes, and HIV. Nearly 25% of people living with HIV/AIDS in the United States are 50 or older (Office on Women’s Health, 2010b). Githens and Abramsohn (2010) found that only 25% of adults 50 and over who were single or had a new sexual partner used a condom the last time they had sex. Robin (2010) stated that 40% of those 50 and over have never been tested for HIV. These results indicate that educating all individuals, not just adolescents, on healthy sexual behavior is important.
Remarriage and Cohabitation. Older adults who remarry often find that their remarriages are more stable than those of younger adults. Kemp and Kemp (2002) suggest that greater emotional maturity may lead to more realistic expectations regarding marital relationships, leading to greater stability in remarriages in later life. Older adults are also more likely to be seeking companionship in their romantic relationships. Carr (2004a) found that older adults who have considerable emotional support from their friends were less likely to seek romantic relationships. In addition, older adults who have divorced often desire the companionship of intimate relationships without marriage. As a result, cohabitation is increasing among older adults, and like remarriage, cohabitation in later adulthood is often associated with more positive consequences than it is in younger age groups (King & Scott, 2005). No longer being interested in raising children and perhaps wishing to protect family wealth, older adults may see cohabitation as a good alternative to marriage. In 2014, 2% of adults aged 65 and up were cohabitating (Stepler, 2016b).
Living Apart Together. In addition to cohabiting, there has been an increase in living apart together (LAT), which is “a monogamous intimate partnership between unmarried individuals who live in separate homes but identify themselves as a committed couple” (Benson & Coleman, 2016, p. 797). This trend has been found in several nations and is motivated by:
- A strong desire to be independent in day-to-day decisions
- Maintaining their own home
- Keeping boundaries around established relationships
- Maintaining financial stability
Besides the desire to be autonomous, there is also a need for companionship, sexual intimacy, and emotional support. According to Bensen and Coleman, there are differences in LAT among older and younger adults. Those who are younger often enter into LAT out of circumstances, such as the job market, and they frequently view this arrangement as a transitional stage. In contrast, 80% of older adults reported that they did not wish to cohabitate or marry. For some, it was a conscious choice to live more independently. For instance, older women desired the LAT lifestyle as a way of avoiding the traditional gender roles that are often inherent in relationships where couples live together. However, some older adults become LATs because they fear social disapproval from others if they were to live together.
Widowhood. With increasing age, women were less likely to be married or divorced but more likely to be widowed, reflecting a longer life expectancy relative to men. About 2 out of 10 women aged 65 to 74 were widowed compared with 4 out of 10 women aged 75 to 84 and 7 out of 10 women 85 and older. More than twice as many women 85 and older were widowed (72 percent) compared to men of the same age (35 percent) (Roberts & Stella, 2016). The death of a spouse is one of life’s most disruptive experiences. It is especially hard on men who lose their wives. Often widowers do not have a network of friends or family members to fall back on and may have difficulty expressing their emotions to facilitate grief. Also, they may have been very dependent on their mates for routine tasks such as cooking, cleaning, etc.
Losing one’s spouse is one of the most difficult transitions in life. The Social Readjustment Rating Scale, commonly known as the Holmes-Rahe Stress Inventory, rates the death of a spouse as the most significant stressor (Holmes & Rahe, 1967). The loss of a spouse after many years of marriage may make an older adult feel adrift in life. They must remake their identity after years of seeing themselves as a husband or wife. Approximately 1 in 3 women aged 65 and older are widowed, compared with about 1 in 10 men.
Widows may have less difficulty because they have a social network and can take care of their own daily needs. They may have more difficulty financially if their husbands have handled all the finances in the past. They are much less likely to remarry because many do not wish to and because there are fewer men available. At 65, there are 73 men for every 100 women. The sex ratio becomes even further imbalanced at 85, with 48 men to every 100 women (Census Bureau, 2011)
Loneliness is the biggest challenge for those who have lost their spouse (Kowalski, et al., 2008). However, several factors can influence how well someone adjusts to this life event. Older adults who are more extroverted (McCrae & Costa, 1988) and have higher self-efficacy (Carr, 2004b) often fare better. Positive support from adult children is also associated with fewer symptoms of depression and better overall adjustment in the months following widowhood (Ha, 2010).
The context of the death is also an important factor in how people may react to the death of a spouse. The stress of caring for an ill spouse can result in a mixed blessing when the ill partner dies (Erber & Szuchman, 2015). The death of a spouse who died after a lengthy illness may come as a relief for the surviving spouse, who may have had the pressure of providing care for someone who was increasingly less able to care for themselves. At the same time, this sense of relief may be intermingled with guilt for feeling relief at the passing of their spouse.
Loneliness or Solitude
Loneliness is the discrepancy between the social contact a person has and the contacts a person wants (Brehm, Miller, Perlman, & Campbell, 2002). It can result from social or emotional isolation. Women tend to experience loneliness due to social isolation, and men from emotional isolation. Loneliness can be accompanied by a lack of self-worth, impatience, desperation, and depression. Being alone does not always result in loneliness. For some, being alone means solitude. Solitude involves gaining self-awareness, taking care of the self, being comfortable alone, and pursuing one’s interests (Brehm et al., 2002). In contrast, loneliness is perceived as social isolation.
For those in late adulthood, loneliness can be especially detrimental. Novotney (2019) reviewed the research on loneliness and social isolation and found that loneliness was linked to a 40% increase in the risk of dementia and a 30% increase in the risk of stroke or coronary heart disease. This was hypothesized to be due to reasons that were both biological (e.g., a rise in stress hormones), psychological (e.g., depression and anxiety), as well as social (e.g., the individual lacks encouragement from others to engage in healthy behaviors). In contrast, older adults who take part in social clubs and church groups have a lower risk of death. Opportunities to reside in mixed-age housing and continue to feel like productive members of society have also been found to decrease feelings of social isolation and, thus, loneliness.
Couples who remarry after midlife tend to be happier in their marriages than in their first marriages. These partners are likely to be more financially independent, have grown children, and enjoy the greater emotional wisdom that comes with experience.
Single, Cohabiting, and Remarried Older Adults
About 6 percent of adults never marry. Many have long-term relationships, however. The never-married tend to be very involved in family and caregiving and do not appear to be particularly unhappy during late adulthood, especially if they have a healthy network of friends. Friendships tend to be an important influence on life satisfaction during late adulthood. Friends may be more influential than family members for many older adults. According to socioemotional selectivity theory, older adults become more selective in their friendships than when they were younger (Carstenson et al., 2003). Friendships are not formed in order to enhance status or careers and may be based purely on a sense of connection or the enjoyment of being together. Most elderly people have at least one close friend. These friends may provide emotional as well as physical support. Being able to talk with friends and rely on others is very important during this stage of life.
About 4 percent of older couples chose cohabitation over marriage (Chevan, 1996). The Pew Research Center reported in 2017 that the number of cohabiters over age 50 rose to 4 million from 2.3 million over the decade and found the number over age 65 doubled to about 900,000 (Stepler, 2017). As discussed in our lesson on early adulthood, these couples may prefer cohabitation for financial reasons, maybe same-sex couples who cannot legally marry or couples who do not want to marry because of previous dissatisfaction with marital relationships.
LBGTQIA+ Older Adults
Approximately 3 million older adults in the United States identify as lesbian or gay (Hillman & Hinrichsen, 2014). By 2025 that number is expected to rise to more than 7 million (National Gay and Lesbian Task Force, 2006). Despite the increase in numbers, older lesbian and gay adults are one of the least researched demographic groups, and the research there portrays a population faced with discrimination.
According to the Centers for Disease Control and Prevention (2011), compared to heterosexuals, lesbian and gay adults experience disparities in both physical and mental health. More than 40% of lesbian and gay adults ages 50 and over suffer from at least one chronic illness or disability, and compared to heterosexuals, they are more likely to smoke and binge drink (Hillman & Hinrichsen, 2014).
Additionally, gay older adults have an increased risk of prostate cancer (Blank, 2005) and infection from HIV and other sexually transmitted illnesses (Centers for Disease Control and Prevention, 2008). When compared to heterosexuals, lesbian and gay elders have less support from others as they are twice as likely to live alone and four times less likely to have adult children (Hillman & Hinrichsen, 2014).
There has been a growth of interest in lesbian, gay, bisexual, transgender, and queer (LGBTQ+) aging in recent years. Many retirement issues for lesbian, gay, bisexual, transgender (LGBT), and intersex people are unique from their non-LGBTI counterparts, and these populations often have to take extra steps to address their employment, health, legal, and housing concerns to ensure their needs are met.
Throughout the United States, there are 1.5 million adults over the age of 65 who identify as lesbian, gay, or bisexual, and two million people above the age of 50 who identify as such. That number is expected to double by 2030, as estimated in a study done by the Institute for Multigenerational Health at the University of Washington. While LGBTQ+ people have increasingly become more visible and accepted into mainstream cultures, LGBTQ+ elders and retirees are still considered a newer phenomenon, which creates both challenges and opportunities as they redefine some commonly held beliefs about aging.
LGBTQ+ individuals are less likely to have strong family support systems in place to have relatives to care for them during aging. They are twice as likely to enter old age living as a single person; and two and a half times more likely to live alone. Because institutionalized homophobia, as well as cultural discrimination and harassment, still exist, they are less likely to access health care, housing, or social services or, when they do, find the experience stressful or demeaning. Joel Ginsberg, executive director of the Gay Lesbian Medical Association, asserts, “Only by pursuing both strategies, encouraging institutional change and encouraging…and empowering individuals to ask for what they want, will we end up with quality care for LGBT people.” (Cassell, 2007).
These older adults have concerns over health insurance and being able to share living quarters in nursing homes and assisted living residences where staff members tend not to be accepting of homosexuality and bisexuality. SAGE (Senior Action in a Gay Environment) is an advocacy group working on remedying these concerns. Same-sex couples who have endured prejudice and discrimination through the years and can rely upon one another continue to have support through late adulthood.
Lesbian and gay older adults who belong to ethnic and cultural minorities, conservative religions, and rural communities may face additional stressors. Ageism, heterocentrism, sexism, and racism can combine cumulatively and impact the older adult beyond the negative impact of each individual form of discrimination (Hillman & Hinrichsen, 2014). David and Knight (2008) found that older gay black men reported higher rates of racism than younger gay black men and higher levels of perceived ageism than older gay white men.
LGBTQ+ Aging Centers have opened in several major metropolitan areas with the goal of training long-term care providers about LGBT-specific issues, an area of frequent discrimination. Legislative solutions are available as well: “California is the only state with a law saying the gay elderly have special needs, like other members of minority groups. A new law encourages training for employees and contractors who work with the elderly and permits state financing of projects like gay senior centers” (Gross, 2007). Twenty states prohibit discrimination in housing and public accommodation on the basis of sexual orientation.
LGBT Elder Care. Approximately 7 million LGBT people over age 50 will reside in the United States by 2030, and 4.7 million of them will need elder care. Decisions regarding elder care are often left to families, and because many LGBT people are estranged from their families and do not have children of their own, they are left in a vulnerable position when seeking living arrangements (Alleccia & Bailey, 2019). A history of discriminatory policies, such as housing restricted to married individuals involving one man and one woman, and stigma associated with LGBT people make them especially vulnerable to negative housing experiences when looking for elder care.

Although lesbian and gay older adults face many challenges, more than 80% indicate that they engage in some form of wellness or spiritual activity (Fredrickson-Goldsen et al., 2011). They also gather social support from friends and “family members by choice” rather than legal or biological relatives (Hillman & Hinrichsen, 2014). This broader social network provides extra support to gay and lesbian elders.
An important consideration when reviewing the development of gay and lesbian older adults is the cohort in which they grew up (Hillman & Hinrichsen, 2014). The oldest lesbian and gay adults came of age in the 1950s when there were no laws to protect them from victimization. The baby boomers, who grew up in the 1960s and 1970s, began to see states repeal laws that criminalized homosexual behavior. Future lesbian and gay elders will have different experiences due to the legal right for same-sex marriage and greater societal acceptance. Consequently, just like all those in late adulthood, understanding that gay and lesbian elders are a heterogeneous population is important when understanding their overall development.
Older Adults, Caregiving, and Long-Term Care

Older adults do not typically relocate far from their previous places of residence during late adulthood. A minority lives in planned retirement communities that require residents to be of a certain age. However, many older adults live in age-segregated neighborhoods that have become segregated as original inhabitants have aged and children have moved on. A major concern in future city planning and development will be whether older adults wish to live in age-integrated or age-segregated communities.
Over 60 million Americans, or 19% of the population, lived in multigenerational households or homes with at least two adult generations in 2016 (Figure 8). It has become an ongoing trend for elderly generations to move in and live with their children, as they can give them support and help with everyday living (Passel & Cohn, 2018).
Most (70 percent) of older adults who require care receive that care in the home. Most are cared for by their spouse or by a daughter or daughter-in-law. However, those who are not cared for at home are institutionalized. In 2008, 1.6 million out of the total 38.9 million Americans age 65 and older were nursing home residents (Census Bureau, 2011). Among 65-74, 11 per 1,000 adults aged 65 and older were in nursing homes. That number increases to 182 per 1,000 after age 85. More residents are women than men, and more are Black than white. As the population of those over age 85 continues to increase, more will require nursing home care. Meeting the psychological and social as well as physical needs of nursing home residents is a growing concern. Rather than focusing primarily on food, hygiene, and medication, the quality of life for the seniors within these facilities is important as well. Residents of nursing homes are sometimes stripped of their identity as their personal possessions and reminders of their lives are taken away. A rigid routine in which the residents have little voice can be alienating to anyone, but more so for an older adult. Routines that encourage passivity and dependence can be damaging to self-esteem and lead to further deterioration of health. Greater attention needs to be given to promoting successful aging within institutions.
Try It
Do those in late adulthood primarily live alone? No. In 2014, of those 65 years of age and older, approximately 72% of men and 46% of women lived with their spouse (Vespa & Schondelmyer, 2014). Between 1900 and 1990, the number of older adults living alone increased, most likely due to improvements in health and longevity during this time (see Figure 9). Since 1990, the number of older adults living alone has declined because older women are more likely to be living with their spouses or children (Stepler, 2016c).

Women continue to make up the majority of older adults living alone in the U.S., although that number has dropped from those living alone in 1990 (Stepler, 2016a). Older women are more likely to be unmarried, living with children, with other relatives or non-relatives. Older men are more likely to be living alone than they were in 1990, although older men are more likely to reside with their spouses. The rise in divorce among those in late adulthood, along with the drop in remarriage rate, has resulted in slightly more older men living alone today than in the past (Stepler, 2016c).
Older adults who live alone report feeling more financially strapped than those living with others (Stepler, 2016d). According to a Pew Research Center Survey, only 33% of those living alone reported they were living comfortably, while nearly 49% of those living with others said they were living comfortably. Similarly, 12% of those living alone, but only 5% of those living with others, reported that they lacked money for basic needs (Stepler, 2016d).
Do those in late adulthood primarily live with family members? No. There are significantly fewer older adults living in multigenerational housing, that is, three generations living together, than in previous generations (Erber & Szuchman, 2015). According to the Pew Research Center (2011) nearly 17% of the population lived in a house with at least two adult generations based on the 2010 census results. However, ethnic differences are noted in the percentage of multigenerational households, with Hispanic (22%), Black (23%), and Asian (25%) families living together in greater numbers than White families (13%). Consequently, with the exception of some cultural groups, the majority of older adults wish to live independently for as long as they are able.
Do those in late adulthood move after retirement? No. According to Erber and Szuchman (2015), the majority of those in late adulthood remain in the same location and often in the same house where they lived before retiring. Although some younger late adults (65-74 years) may relocate to warmer climates, once they are older (75-84 years), they often return to their home states to be closer to adult children (Stoller & Longino, 2001). Despite the previous trends, however, the recent housing crisis has kept those in late adulthood in their current suburban locations because they are unable to sell their homes (Erber & Szuchman, 2015).
Do those in late adulthood primarily live in institutions? No. Only a small portion (3.2%) of adults older than 65 lived in an institution in 2015 (Administration on Aging, 2016). However, as individuals increase in age the percentage of those living in institutions, such as a nursing home, also increases. Specifically: 1% of those 65-74, 3% of those 75-84, and 10% of those 85 years and older lived in an institution in 2015. Due to the increasing number of baby boomers reaching late adulthood, the number of people who will depend on long-term care is expected to rise from 12 million in 2010 to 27 million in 2050 (United States Senate Commission on Long-Term Care, 2013). To meet this higher demand for services, a focus on the least restrictive care alternatives has resulted in a shift toward home and community-based care instead of placement in a nursing home. (Gatz et al., 2016).
Putting it all Together

The period of late adulthood, which starts around age 65, is characterized by great changes and ongoing personal development. Older adults face profound physical, cognitive, and social changes, and many figure out strategies for adjusting to them and successfully coping with old age. In late adulthood, people begin the decline that will be part of their lives until death. The declines in the senses—vision, hearing, taste, and smell—can have major psychological consequences. Most illnesses and diseases of late adulthood are not particular to old age, but the incidences of cancer and heart disease rise with age. People in late adulthood are also more prone to develop arthritis, hypertension, major neurocognitive disorders, and Alzheimer’s disease. Proper diet, exercise, and avoidance of health risks can all lead to overall well-being during old age, and sexuality can continue throughout the lifespan in healthy adults. Thus, many older adults can maintain physical and mental strength until they die, and their social worlds can also remain as vital and active as they want.
Cognitively, we find that older people adjust quite well to the challenges of aging by adopting new strategies for solving problems and compensating for loss of abilities. Although some intellectual abilities gradually decline throughout adulthood, starting at around the age of 25, others stay relatively steady. For example, research shows that while fluid intelligence declines with age, crystallized intelligence remains steady and may even improve in late adulthood. Many cognitive abilities can be maintained with stimulation, practice, and motivation. Declines in memory mainly affect episodic memory, short-term memory, or working memory. Explanations of memory changes in old age focus on environmental factors, information processing declines, and biological factors. Due to this perceived loss of abilities by others, older people are often subject to ageism or prejudice and discrimination against people based on their age.
Socially, many older adults become adept at coping with the changes in their lives, such as the death of a spouse and retirement from work. Erikson calls older adulthood the integrity vs. despair stage. According to Erikson, individuals in late adulthood engage in looking back over their lives, evaluating their experiences, and coming to terms with decisions. Other theorists focus on the tasks that define late adulthood and suggest that older people can experience liberation and self-regard. Marriages in older adulthood are generally happy, but the many changes in late adulthood can cause stress, which may result in divorce. The death of a spouse has major psychological, social, and material effects on the surviving widow and makes the formation and continuation of friendships highly important. Family relationships are a continuing part of most older people’s lives, especially relationships with siblings, children, and grandchildren. Friendships, an important source of social support, are not only valued but needed in late adulthood.
Whether death is caused by genetic programming or by general physical wear-and-tear is an unresolved question. Life expectancy, which has risen for centuries, varies with gender, race, and ethnicity, and new approaches to increasing life expectancy are a growing research topic.
Supplemental Materials
Websites
-
Classification of Neurocognitive Disorders in DSM-5: A Work in Progress
- This article explains the shift in renaming the term dementia to neurocognitive disorders. The Neurocognitive Disorders Work Group of the American Psychiatric Association’s (APA) DSM-5 Task Force began work in April 2008 on their task of proposing revisions to the criteria for the disorders referred to in DSM-IV as Delirium, Dementia, Amnestic, and Other Cognitive Disorders.
- American Society on Aging
- ASA is the go-to source for cultivating leadership, advancing knowledge, and strengthening the skills of our members and others who work with and on behalf of older adults.
Videos
- Studying brains as we age
- Learn more about how psychology research is conducted through the work of a neuropsychologist who studies how cultural experiences affect our brains as we age. Closed captioning is available.
- Crash Course Video #14 – Remembering and Forgetting
- This video on remembering and forgetting includes information on topics such as implicit and explicit memory, encoding, retrieval, and the misinformation effect. Closed captioning is available.
- 57 Years Apart – A Boy And a Man Talk About Life
- We brought together two people with a very large gap of 57 years between them and got them to ask each other questions about life and growing up. Our aim was to see if people from opposing stages of their lives could learn from each other.
- Life Lessons From 100-Year-Olds
- We asked three centenarians about their most valuable life lessons and regrets. The conversations that followed were remarkable. They talked about the importance of family, people, relationships, and love. Their view on life as elderly citizens with a lot of experience is truly inspiring and motivating. Enjoy the video!
- What is Alzheimer’s disease? – Ivan Seah Yu Jun
- Alzheimer’s disease is the most common cause of dementia, affecting over 40 million people worldwide. And though it was discovered over a century ago, scientists are still grappling for a cure. Ivan Seah Yu Jun describes how Alzheimer’s affects the brain, shedding light on the different phases of this complicated, destructive disease.
- How Old Are Your Ears? (Hearing Test)
- How high can you hear? Take this ‘test’ to see how old your ears are!
- Life and Death in Assisted Living
- More and more elderly Americans are choosing to spend their later years in assisted living facilities, which have sprung up as an alternative to nursing homes. But is this loosely regulated, multi-billion dollar industry putting seniors at risk? In a major investigation with ProPublica, FRONTLINE examines the operations of the nation’s largest assisted living company, raising questions about the drive for profits and fatal lapses in care.
- This TED Talk defines ageism and discusses the impacts of ageist thinking and structures and ways to disrupt it.
- This short interview with Dr. David Williams discusses how racism shows up in the medical profession and the importance of combatting it.
- This link connects to Healthy People 2030, a government initiative to improve health for everyone. It has an excellent section on social determinants of health. https://health.gov/healthypeople
- This link connects to the Illinois Alliance for Welcoming Health Care, which brings together healthcare providers and community organizations to reach out to underserved immigrant communities. https://www.ilalliancehealth.org
- This TED talk discusses the four phases of a satisfying and productive retirement. https://www.youtube.com/watch?v=DMHMOQ_054U
- This TED Talk discusses the impact of menopause on brains.
Attributions
Human Growth and Development by Ryan Newton is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License,
Individual and Family Development, Health, and Well-being by Diana Lang, Nick Cone; Laura Overstreet, Stephanie Loalada; Suzanne Valentine-French, Martha Lally; Julie Lazzara, and Jamie Skow is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License,
Human Development by Human Development Teaching & Learning Group under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License,
References
Administration on Aging. (2021). A profile of older Americans, 2020. https://acl.gov/sites/default/files/Aging%20and%20Disability%20in%20America/2020ProfileOlderAmericans.Final_.pdf
Alleccia, J., & Bailey, M. (2019, June 12). A concern for LGBT boomers. The Chicago Tribune, pp. 1-2.
Alterovitz, S. S., & Mendelsohn, G. A. (2011). Partner preferences across the lifespan: Online dating by older adults. Psychology of Popular Media Culture, 1, 89-95.
American Psychological Association. (n.d.) African American older adults and race-related stress: How aging and health-care providers can help. https://www.apa.org/pi/aging/resources/african-american-stress.pdf.
Antonucci, T. C. (2001). Social relations: An examination of social networks, social support and sense of control. In J.E. Birren & K. W. Schaie (Eds.), Handbook of the psychology of aging (5th ed., pp. 427–453). New York: Academic Press.
Beit-Hallahmi, B., & Argyle, M. (1998). Religious behavior, belief, and experience. New York: Routledge.
Berger, K. S. (2005). The developing person through the life span (6th ed.). New York: Worth.
Berk, L. (2007). Development through the life span (4th ed.). Boston: Allyn and Bacon.
Blanchard-Fields, F. (2007). Everyday problem solving and emotion: An adult development perspective. Current Directions in Psychoogical Science, 16, 26–31
Bookwala, J., Marshall, K. I., & Manning, S. W. (2014). Who needs a friend? Marital status transitions and physical health outcomes in later life. Health Psychology, 33(6), 505-515.
Brehm, S. S., Miller, R., Perlman, D., & Campbell, S. (2002). Intimate relationships (3rd ed.). Boston: McGraw-Hill Higher Education.
Carr, D. (2004a). The desire to date and remarry among older widows and widowers. Journal of Marriage and Family, 66, 1051– 1068.
Carr, D. (2004b). Gender, preloss marital dependence, and older adults’ adjustment to widowhood. Journal of Marriage and Family, 66, 220-235.
Carstensen, L. L. (1993). Motivation for social contact across the life span: A theory of socioemotional selectivity. In J. E. Jacobs (Ed.), Nebraska Symposium on Motivation, 1992: Developmental perspectives on motivation (pp. 209–254). Lincoln, NE: University of Nebraska Press.
Carstensen, L. L., Gottman, J. M., & Levensen, R. W. (1995). Emotional behavior in long-term marriage. Psychology and Aging, 10, 140–149.
Carstensen, L. L., Isaacowitz, D. M., & Charles, S. T. (1999). Taking time seriously: A theory of socioemotional selectivity. American Psychologist, 54, 165–181.
Cassell, H. (2007). “LGBT Health Care Movement Gains Momentum”. Bay Area Reporter. https://www.ebar.com/news///238394
Cherlin, A. J., & Furstenberg, F. F. (1986). The new American grandparent: A place in the family, a life apart. New York: Basic Books.
Cumming, E., & Henry, W. E. (1961). Growing old: Process of disengagement. Basic Books.
Davidson, K. (2001). Late life widowhood, selfishness and new partnership choices: A gendered perspective. Ageing and Society, 21, 297–317.
De Vaus, D. & McAllister, I. (1987). Gender differences in religion: A test of the structural location theory. American Sociological Review, 52, 472-481.
de Vries, B. (1996). The understanding of friendship: An adult life course perspective. In C. Magai & S. H. McFadden (Eds.), Handbook of emotion, adult development, and aging (pp. 249–268). San Diego, CA: Academic Press.
Erber, J. T., & Szuchman, L. T. (2015). Great myths of aging. West Sussex, UK: John Wiley & Sons.
Erikson, E. H. (1959). Identity and the life cycle: Selected papers. Psychological Issues, 1, 1–171. ↵
Erikson, E. H. (1980). Identity and the life cycle. W W Norton & Co.
Fingerman, K. L., & Birditt, K. S. (2011). Relationships between adults and their aging parents. In K. W. Schaie & S. I Willis (Eds.). Handbook of the psychology of aging (7th ed.) (pp 219-232). SanDiego: Elsevier Academic Press.
Fischer, C. S. (1982). To dwell among friends: Personal networks in town and city. Chicago, IL: University of Chicago Press.
Fox, S. (2004). Older Americans and the Internet. PEW Internet & American Life Project. http://www.pewinternet.org/report_display.asp?r_117
Fredriksen-Goldsen, K. I., Kim, H. J., Emlet, C. A., Muraco, A., Erosheva, E. A., Hoy-Ellis, C. P.,… Petry, H. (2011). The aging and health report: disparities and resilience among lesbian, gay, bisexual, and transgender older adults. Seattle, WA: Institute for Multigenerational Health.
Garrett, B. (2015). Brain and behavior (4th ed.) Thousand Oaks, CA: Sage.
Gatz, M., Smyer, M. A., & DiGilio, D. A. (2016). Psychology’s contribution to the well-being of older Americans. American Psychologist, 71(4), 257-267.
George, L.K. (2009). Still happy after all these years: research frontiers on subjective well-being in later life. Journal of Gerontology: Social Sciences, 65B (3), 331–339. doi:10.1093/geronb/gbq006
Githens, K., & Abramsohn, E. (2010). Still got it at seventy: Sexuality, aging, and HIV. Achieve, 1, 3-5.
Glaser, K., Stuchbury, R., Tomassini, C., & Askham, J. (2008). The long-term consequences of partnership dissolution for support in later life in the Unites Kingdom. Ageing & Society, 28(3), 329-351.
Goyer, A. (2010). More grandparents raising grandkids: New census data shows and increase in children being raised by extended family. AARP. http://www.aarp.org/relationships/grandparenting/info-12- 2010/more_grandparents_raising_grandchildren.html
Greenfield, E. A., Vaillant, G. E., & Marks, N. F. (2009). Do formal religious participation and spiritual perceptions have independent linkages with diverse dimensions of psychological well-being? Journal of Health and Social Behavior, 50, 196-212.
Gross, J. (2007). “Aging and Gay, and Facing Prejudice in Twilight”. The New York Times. https://www.nytimes.com/2007/10/09/us/09aged.html
Gusky, J. (2012). Why aren’t they screaming? A counselor’s reflection on aging. Counseling Today. Retrieved from https://ct.counseling.org/2012/04/why-arent-they-screaming-a-counselors-reflection-on-aging/
Ha, J. H. (2010). The effects of positive and negative support from children on widowed older adults’ psychological adjustment: A longitudinal analysis. Gerontologist, 50, 471-481.
Havey, Elizabeth A. (2015). “What’s Generativity and Why It’s Good for You.” Huffington Post. Retrieved from https://www.huffpost.com/entry/whats-generativity-and-why-its-good-foryou_b_7629174?guccounter=1&guce_referrer=aHR0cHM6Ly93d3cuZ29vZ2xlLmNvbS8&guce_referrer_sig=AQAAAISJrz_B9ylovtOxRuUNpAiqtA6GZvMM8nUxuyG0eL1AwbMX0F2fEIL6QyV_cF4SYXbn9OyhdIzXtdHB-UwJqn73I0rFzpLKpv35gT
Havighurst, R. J., Albrecht, R. E. (1953) Older people. Longmans: Green, New York
He, W., Goodkind, D., & Kowal, P. (2016). An aging world: 2015. International Population Reports. U.S. Census Bureau.
He, W., Sengupta, M., Velkoff, V., & DeBarros, K. (2005.). U. S. Census Bureau, Current Popluation Reports, P23-209, 65+ in the United States: 2005 (United States, U. S. Census Bureau). http://www.census.gov/prod/1/pop/p23- 190/p23-190.html
Hillman, J., & Hinrichsen, G. A. (2014). Promoting and affirming competent practice with older lesbian and gay adults. Professional Psychology: Research and Practice, 45(4), 169-277.
Holmes, T. H., & Rahe, R. H. (1967). The social readjustment rating scale. Journal of psychosomatic research, 11, 213.
Hooyman, N. R., & Kiyak, H. A. (2011). Social gerontology: A multidisciplinary perspective (9th Ed.). Boston, MA: Pearson
Jarrett, C. (2015). Great myths of the brain. West Sussex, UK: John Wiley & Sons.
Kahn, R. L., & Antonucci, T. C. (1980). Convoys over the life course: Attachment, roles, and social support. In P. B. Baltes & O. Brim (Eds.) Life-span development and behavior (Vol. 3, pp. 253-286). New York: Academic Press.
Kaskie, B., Imhof, S., Cavanaugh, J., & Culp, K. (2008). Civic engagement as a retirement role for aging Americans. The Gerontologist, 48, 368-377.
Kahana, E., Bhatta, T., Lovegreen, L. D., Kahana, B., & Midlarsky, E. (2013). Altruism, helping, and volunteering: Pathways to well-being in late life. Journal of Aging and Health, 25(1), 159-187.
Kemp, E. A., & Kemp, J. E. (2002). Older couples: New romances: Finding and keeping love in later life. Berkeley, CA: Celestial Arts.
King, V., & Scott, M. E. (2005). A comparison of cohabitating relationships among older and younger adults. Journal of Marriage and Family, 67(2), 271-285.
Kolb, B., & Whishaw, I. Q. (2011). An introduction to brain and behavior (3rd ed.). New York, NY: Worth Publishers.
Kowalski, S. D., & Bondmass, M. D. (2008). Physiological and psychological symptoms of grief in widows. Research in Nursing and Health, 31(1), 23-30.
Krause, N. (2012). Meaning in life and healthy aging. In P. T. P. Wong (Ed.), The human quest for meaning: Theories, research and application (2nd ed., pp. 409-432). New York, NY: Routledge
Kowalski, S. D., & Bondmass, M. D. (2008). Physiological and psychological symptoms of grief in widows. Research in Nursing of Elder Abuse and Neglect, 26, 207-222. and Health, 31(1), 23-30.
Lang, F. R., & Schütze, Y. (2002). Adult children’s supportive behaviors and older adults’ subjective well-being: A developmental perspective on intergenerational relationships. Journal of Social Issues, 58, 661-680.
Lee, S. J., Steinman, M., & Tan, E. J. (2011). Volunteering, driving status, and mortality in U.S. retirees. Journal of the American Geriatric Society, 59(2), 274-280. https://doi.org/10.1111/j.1532-5415.2010.03265x
Lin, I. F. (2008). Consequences of parental divorce for adult children’s support of their frail parents. Journal of Marriage and Family, 70(1), 113-128.
Livingston, G. (2019). Americans 60 and older are spending more time in front of their screens than a decade ago. Retrieved from: https://www.pewresearch.org/fact-tank/2019/06/18/americans-60-and-older-are-spending-more-time-in-front-of- their-screens-than-a-decade-ago/
McCrae, R. R., & Costa, P. T. (1988). Physiological resilience among widowed men and women: A 10 year follow-up study of a national sample. Journal of Social Issues, 44(3), 129-142.
McDonald, L., & Robb, A. L. (2004). The economic legacy of divorce and separation for women in old age. Canadian Journal on Aging, 23, 83-97.
National Gay and Lesbian Task Force. (2006). Make room for all: Diversity, cultural competency and discrimination in an aging America. Washington, DC: The Policy Institute of the National Gay and Lesbian Task Force.
Nelson, T. D. (2016). Promoting healthy aging by confronting ageism. American Psychologist, 71(4), 276-282.
Newsroom: Facts for Features & Special Editions: Facts for Features: Older Americans Month: May 2010. (2011, February 22). Census Bureau Home Page. http://www.census.gov/newsroom/relea…cb10-ff06.html
Nilsson, H., Bülow, P. H., & Kazemi, A. (2015). Mindful sustainable aging: Advancing a comprehensive approach to the challenges and opportunities of old age. Europe’s Journal of Psychology, 11(3), 494–508. https://doi.org/10.5964/ejop.v11i3.949
Novotney, A. (2019). Social isolation: It could kill you. Monitor on Psychology, 50(5), 33-37. Office on Women’s Health. (2010a). Raising children again. Retrieved from http://www.womenshealth.gov/aging/caregiving/raising-children-again.html
Office on Women’s Health. (2010a). Raising children again. http://www.womenshealth.gov/aging/caregiving/raising-children-again.html
Office on Women’s Health. (2010b). Sexual health. Retrieved from http://www.womenshealth.gov/aging/sexual-health/
Overstreet, L. (2006). Unhappy birthday: Stereotypes in late adulthood. Unpublished manuscript, Texas Woman’s University.
Papernow, P. L. (2018). Recoupling in midlife and beyond: From love at last to not so fast. Family Processes, 57(1), 52-69.
Passel, J. & Cohn, D. (2018). A record 64 million Americans live in multigenerational households. Pew Research Center. https://www.pewresearch.org/fact-tank/2018/04/05/a-record-64-million-americans-live-in-multigenerational-households/.
Perry, T. E., Ruggiano, N., Shtompel, N., & Hassevoort, L. (2015). Applying Erikson’s wisdom to self-management practices of older adults: findings from two field studies. Research on Aging, 37(3), 253–274. doi:10.1177/0164027514527974
Pew Research Center. (2011). Fighting poverty in a tough economy. Americans move in with their relatives. Retrieved from http://www.pewsocialtrends.org/files.2011/10.Multigenerationsl-Households-Final1.pdf
Riediger, M., Freund, A.M., & Baltes, P.B. (2005). Managing life through personal goals: Intergoal facilitation and intensity of goal pursuit in younger and older adulthood. Journals of Gerontology, 60B, P84-P91.
Robin, R. C. (2010). Grown-up, but still irresponsible. New York Times. http://www.nytimes.com/2010/10/10weekinreview/10rabin.html>.
Robins, R.W., & Trzesniewski, K.H. (2005). Self-esteem development across the lifespan. Current Directions in Psychological Science, 14 (3), 158-162. DOI: 10.1111/j.0963- 7214.2005.00353x
Roberts, A. & Stella, O. U. (2016). The Population 65 Years and Older in the United States: 2016 American Community Survey Reports. https://www.census.gov/content/dam/Census/library/publications/2018/acs/ACS-38.pdf
Rubinstein, R.L. (2002). The third age. In R.S. Weiss & S.A. Bass (Eds.), Challenges of the third age; Meaning and purpose in later life (pp. 29-40). New York: Oxford University Press.
Ruckenhauser, G., Yazdani, F., & Ravaglia, G. (2007). Suicide in old age: Illness or autonomous decision of the will? Archives of Gerontology and Geriatrics, 44(6), S355-S358.
Smith, J. (2000). The fourth age: A period of psychological mortality? Max Planck Forum, 4, 75-88. Social Security Administration. (2016). Retirement planner: Benefits by year of birth. Retrieved from https://www.ssa.gov/planners/retire/agereduction.html
Stepler, R. (2016b). Living arrangements of older adults by gender. Pew Research Center Retrieved from http://www.pewsocialtrends.org/2016/02/18/2-living-arrangements-of-older-americans-by-gender/
Stepler, R. (2017). Number of U.S. adults cohabiting with a partner continues to rise, especially among those 50 and older. Pew Research Center. https://www.pewresearch.org/fact-tank/2017/04/06/number-of-u-s-adults-cohabiting-with-a-partner-continues-to-rise-especially-among-those-50-and-older/
Strough, J., Hicks, P. J., Swenson, L. M., Cheng, S., & Barnes, K. A. (2003). Collaborative everyday problem solving: Interpersonal relationships and problem dimensions. International Journal of Aging and Human Development, 56, 43- 66.
Subramanian, S. V., Elwert, F., & Christakis, N. (2008). Widowhood and mortality among the elderly: The modifying role of neighborhood concentration of widowed individuals. Social Science and Medicine, 66, 873-884.
Sullivan, A. R., & Fenelon, A. (2014). Patterns of widowhood mortality. Journal of Gerontology Series B: Psychological and Social Sciences, 69B, 53-62.
Tentori, K., Osherson, D., Hasher, L., & May, C. (2001). Wisdom and aging: Irrational preferences in college students but not older adults. Cognition, 81, B87–B96.
United States Census Bureau. (2014a). American Community Survey, 2014 Estimates: table B10001. http://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?pid=ACS_14_5YR_B10001&prodType=table
United States, National Center for Health Statistics. (2002). National Vital Statistics Report, 50(16). http://www.cdc.gov/nchs/data/dvs/LCWK1_2000.pdf
United States Senate Commission on Long-Term Care. (2013). Report to the Congress. Washington, DC: U. S. Government Printing Office.
Uscher, J. (2006, January). How to make a world of difference-without leaving home. AARP The Magazine – Feel Great. Save Money. Have Fun. Retrieved May 07, 2011, from http://www.aarpmagazine.org/lifestyl…unteering.html
Vaillant, G. E. (2008). Spiritual evolution: A scientific defense of faith. New York: Doubleday Broadway.
Vespa, J. & Schondelmyer, E. (2014). A gray revolution in living arrangements. http://blogs.census.gov/2015/07/14/a-gray-revolution-in-living-arrangements/
Watson, W. K., & Stelle, C. (2011). Dating for older women: Experiences and meanings of dating in later life. Journal of Women and Aging, 23, 263-275.
Wilcox, B. J. Wilcox, D. C., & Ferrucci, L. (2008). Secrets of healthy aging and longevity from exceptional survivors around the globe: Lessons from octogenarians to supercentenarians. Journal of Gerontology, 63(11), 1181-1185.
Wright, K. B., & Query, J. L. (2004). Online support and older adults: A theoretical examination of benefits and limitations of computer-mediated support networks for older adults and possible health outcomes. In J. Nussbaum & J. Coupland (Eds.), Handbook of communication and aging research (2nd ed., pp. 499–519). Mahwah, NJ: Erlbaum.
Wrzus, C., Hanel, M., Wagner, J., & Neyer, F. J. (2013). Social network changes and life events across the lifespan: A meta-analysis. Psychological Bulletin, 139(1), 53-80.
Wu, Z., & Schimmele, C. M. (2007). Uncoupling in late life. Generations, 31(3), 41-46.

{kind=link}