1
Learning Objectives
- Describe the process of confirming pregnancy and estimating the due date (estimated date of birth, [EDB]).
- Evaluate adequacy and patterns of weight gain during different stages of pregnancy.
- Discuss the physical, psychosocial, cultural and behavioral changes occurring as the mother and other family members adapt to pregnancy.
- Outline a plan of care for a pregnant woman experiencing the discomforts of pregnancy.
- Describe assessment measures to determine maternal and fetal well-being in first, second, and third trimesters.
Signs of Pregnancy
- Presumptive
- Presumptive signs of pregnancy are subjective and changes with each experience. Therefore this is not proof of pregnancy. The following are presumptive signs of pregnancy:
- Amenorrhea (earliest symptom), nausea and vomiting with “morning sickness” from 6 to 12 weeks due to the elevation in human chorionic gonadotropin (hCG) levels, urinary frequency, excessive fatigue and quickening. (Kelsey & Nagtalon-Ramos, 2020)

Fetal Movements – may be experienced between 14-22 weeks
- Amenorrhea (earliest symptom), nausea and vomiting with “morning sickness” from 6 to 12 weeks due to the elevation in human chorionic gonadotropin (hCG) levels, urinary frequency, excessive fatigue and quickening. (Kelsey & Nagtalon-Ramos, 2020)
- Presumptive signs of pregnancy are subjective and changes with each experience. Therefore this is not proof of pregnancy. The following are presumptive signs of pregnancy:
- Probable
- Probable signs of pregnancy are objective changes that the examiner (Nurse, Nurse Practitioner, or Medical Practitioner) can detect. These changes include enlargement of the abdomen with continued amenorrhea, Braxton-hicks contractions, uterine soufflé, a positive pregnancy test and palpable fetal outline. At term, the cervical strength is 1/12 of its pre-pregnant strength facilitating the cervical changes during labor. Probable signs of pregnancy can have false positive results in some cases if the client is on infertility medications, has ovarian cysts, or gestational trophoblastic disease. Additionally, changes within the pelvic organs may occur as well and is caused by increased vascular congestion:
- Softening of the cervix (Goodell’s Sign)
- Softening of the isthmus of uterus (Hegar’s Sign)
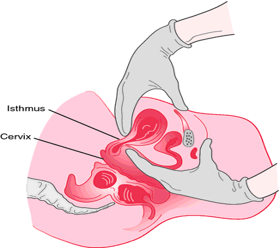
- Purple/bluish discoloration of the vaginal walls and cervix (Chadwick’s Sign)
- Probable signs of pregnancy are objective changes that the examiner (Nurse, Nurse Practitioner, or Medical Practitioner) can detect. These changes include enlargement of the abdomen with continued amenorrhea, Braxton-hicks contractions, uterine soufflé, a positive pregnancy test and palpable fetal outline. At term, the cervical strength is 1/12 of its pre-pregnant strength facilitating the cervical changes during labor. Probable signs of pregnancy can have false positive results in some cases if the client is on infertility medications, has ovarian cysts, or gestational trophoblastic disease. Additionally, changes within the pelvic organs may occur as well and is caused by increased vascular congestion:
- Positive
- Positive signs of pregnancy are conclusive proof that the client is pregnant. These signs of pregnancy include a fetal heartbeat between 120-160 beats per minute (bpm) which can be heard via doppler at approximately 10-12 weeks and by ultrasound, fetal movement detected by the examiner and visualization of the fetus via transvaginal or abdominal ultrasound.
Clinical Pregnancy Testing
Based on the analysis of maternal blood or urine (Lab or OTC)
- Blood Tests (Lab) – can be detected as early as 7-8 days before the missed period.
- Urine Tests 95% accuracy – accurate if testing is completed on the day of expected period, early in the morning midstream collection, can detect low levels of hCG.
Physical Changes in Pregnancy

Uterus:
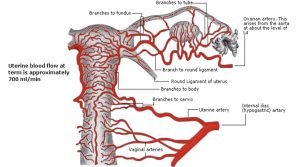
Enlargement of the uterus is the result of hypertrophy and hyperplasia of the myometrial cells. Initial changes in size are caused by increased estrogen and progesterone levels, not by enlarging fetus. After three months, enlargement is due to the growing fetus. Braxton-hicks contractions occur intermittently throughout pregnancy after the fourth month and are consistent with irregular contractions, stimulation from the movement of blood through the placenta. In late pregnancy, these can be uncomfortable and confused with true labor contractions. During the development of the fetus further changes within the uterus include the increase of blood flow through the uterus, increasing by ten-fold. By term, one sixth of the total maternal blood volume is contained in the uterus and the rate of blood flow is between 450-650 ml/minute.
Cervix:
Estrogen induced changes cause endocervical glands to secrete thick, tenacious mucus which accumulates and forms a mucous plug (operculum). The mucous plug seals the cervical canal and prevents ascent of bacteria into the uterus. When cervical dilation begins the mucous plug is expelled.
Ovaries:
Ovaries cease ovum production during pregnancy. Human chorionic gonadotropin (hCG) produced by the fertilized egg maintains the corpus luteum. The corpus luteum secretes progesterone until mid pregnancy at which the placenta then begins to produce progesterone to help sustain the pregnancy to full term.
Vagina:
Estrogen induced changes cause increased vascularization, hyperplasia and hypertrophy of the vagina. Additionally, leucorrhea or vaginal secretions that become thicker, white and more acidic contribute to the creation of the mucous plug. This environment helps to prevent infections but favors yeast and could contribute to an increase in yeast infections during pregnancy. By term, the vaginal wall becomes relaxed to permit distention and passage of the infant.
Breasts:
The breasts will increase in size as a result from glandular hyperplasia which is caused by estrogen and progesterone in preparation for lactation. An increase in pigmentation of the areola may occur. The sebaceous glands, called Montgomery tubercles will hypertrophy and the development of striae on the breast may occur as the pregnancy progresses. Colostrum which is an antibody rich secretion may be expressed by the sixteenth week of pregnancy. The colostrum, being a rich yellow color is often referred to as liquid gold due to its importance in helping with the development of the newborns immunity. Additionally, evidence shows that colostrum can be harvested and stored during the antenatal months of pregnancy.
Respiratory:
Oxygen consumption during pregnancy increases to meet the needs of the mother, fetus, and placenta. Hyperventilation during pregnancy is caused by an increased tidal volume due to the increased oxygen needs and decreased threshold for CO2, this causes mild respiratory alkalosis and may be perceived by the client as having shortness of breath. Respirations are normally between 12 and 22 breaths/minute. The diaphragm will become elevated as a result of the pressure from the enlarging uterus. The chest circumference my increase as much a 6 centimeters. In addition to these changes the client may experience nasal stuffiness, congestion and epistaxis. All a result of estrogen induced edema and vascular congestion of the nasal mucosa.
Cardiovascular:
The heart is pushed up and to the left by the enlarging uterus, and a systolic murmur may be heard in approximately 90% of pregnant women. Throughout the pregnancy blood volume increases by 30-45 % above non-pregnant levels. The cardiac output begins to increase in pregnancy and reaches 30-50% by 32 weeks gestation. The heart rate mildly increases approximately 10-15 beats per minute (bpm) compared to the normal range of 60-90 bpm. The blood pressure typically decreases slightly during the second trimester, with a gradual return to prepregnancy baseline levels by the end of the third trimester. Normal blood pressure remains <135/85.
Physical changes that occur to the cardiovascular system during pregnancy include an increase in the erythrocytes and plasma levels. An increase in erythrocytes is needed for the transport of additional oxygen. The plasma volume increases by 50% which can cause a hemodilution and physiologic anemia of pregnancy due to the plasma volume being greater than the red blood cells. Hematocrit levels are also slightly lower during pregnancy. The risk for anemia can occur during pregnancy and is defined as:
- First & third trimester – <11.0 MG/DL HGB
- Second trimester – <10.5 MG/DL HGB
White blood cell production increases, the increase is unknown why it occurs and WBC counts can be between 5,000 – 15,000/MM3. The pregnant client is in a hypercoagulable state increasing the risk for thromboembolic disease up to six fold. Additional strain can be placed on the client that works long hours in a seated and standing position.
Gastrointestinal:
During the pregnancy a number of changes will occur with the gastrointestinal system in relation to the growth of the fetus, uterus and hormonal changes (Mattson & Smith, 2016). The pregnant client my experience feelings of nausea and vomiting which typically takes place in the first trimester as a result of the increased hCG secretion and changes in carbohydrate metabolism. Additionally, the client may experience an increase in pyrosis (heartburn). This can be in part due to the pressure of the enlarging uterus, elevation of progesterone levels causing relaxation of the smooth muscle, intestines’ displacement laterally, the stomach is displaced superiorly, and the reflux of acidic secretions due to a relaxation of the cardiac sphincter.
Nutritional Needs for A Healthy Pregnancy & Fetal Development
- Carbohydrates – needed for energy and proper bowel function.
- Whole grains, fruits, vegetables and dairy products.
- Proteins- needed to provide amino acids for fetal development & blood volume expansion
- Lean meats, poultry, fish (low mercury), dairy, nuts, legumes
- Fats – essential fatty acids (Omega-3s) needed for CNS development
- Oils, butter, avocado, nuts.
- Calcium & Phosphorus – mineralization of fetal bones & teeth
- Dairy, nuts, figs, dark green leafy vegetables
- Iron – growth of the fetus, placenta & expansion of blood volume
- Lean meats, dark leafy vegetables, eggs, whole grains, dried fruits
- Folic Acid- prevention of neural tube defects, normal growth & lactation and prevents macrocytic, megaloblastic anemia of pregnancy
- Green leafy vegetables, liver, peanuts, whole grain bread & cereal.
Additional gastrointestinal changes include:
- bloating and constipation due to delays in gastric emptying
- hemorrhoids from an increase in the pressure of vessels below the uterus and constipation
- bleeding gums the tissue becomes hyperemic as a result of estrogen.
- ptyalism (tahy–uh-liz-uhm) which is increased salivation
- pruritus which is simply a result of stretching or dry skin.
- Decreased gallbladder emptying can cause a retention of bile salts leading to intense itching. *
Intense Itching
This intense itching can be a signal of a serious disorder called cholestasis of pregnancy. Cholestasis of pregnancy requires medication and/or deliver of the baby at 37 weeks. This is characterized by generalized itching starting with palms of hands & soles of feet. No long-term sequelae for the pregnant client, but it can cause sudden fetal death.
- Decreased gallbladder emptying can cause a retention of bile salts leading to intense itching. *
Urinary Tract:
The growing fetus puts pressure on the bladder causing urinary frequency in both the first and third trimester. This pressure can impair drainage making the pregnant client more susceptible to infection and trauma. Dilation of the kidneys and ureter, usually on the right side due to the lie of the uterus can also lead to urinary stasis and increasing the risk for infection. An increase in glomerular filtration rate results in a decrease of serum creatinine, BUN and uric acid. Due to the inability of the kidney’s to reabsorb all the filtered glucose leading to glycosuria. Glycosuria should be differentiated from gestational diabetes.
Integumentary:
Changes in skin pigmentation occur due to increased estrogen, progesterone, and melanocyte-stimulating hormone levels. The most commonly affected areas include the areolae, nipples, vulva and linea alba. The pregnant client may experience a dark line in the midline of the abdomen (linea nigra), melasma or cholasma (“Mask of Pregnancy”) which effects the cheeks, forehead and nose, and stretch marks (striae). In some severe cases a pregnant client can present with pruritic urticarial papules and plaques of pregnancy (PUPPP). PUPPP causes are unknown, but can be extremely uncomfortable for the client, treatment options are also limited.
Musculoskeletal:
The release of the hormones relaxin and progesterone can cause relaxation of the pelvic joints to help aid in the delivery of the fetus. This may lead to a change in gain and cause the appearance of waddling, it can also cause round ligament pain. The pregnant clients center of gravity will also shift with the enlarging uterus causing a an accentuated curve in the lumbodorsal spine and posture changes leading to complaints of backaches. In some instances pressure from the enlarging uterus can cause a separation of the rectus abdominis muscle (diastis recti). Severe separation can affect subsequent support for future pregnancies.
Nervous System:
Due to the release of multiple hormones and changes physically during the pregnancy, the client may experience problems with their sleep patterns. They may experience difficulty falling asleep, frequent awakenings, active fetus and nocturia. Additionally, the pregnant client may experience a decrease in their attention, concentration and memory. With increases in the blood volume and changes in the vascular system the client may exhibit an exacerbation of carpal tunnel syndrome and sciatica. Being at higher risk of hypocalcemia and or dehydration the pregnant client may also experience an increase in muscle cramps.
Endocrine:
Several changes occur to the endocrine system during pregnancy and can have an impact on the growth and development of the fetus. An increase in T4 production occurs due to an increase in vascularity and hyperplasia of the thyroid gland. The pituitary gland enlarges and supports the pregnancy through the secretion of several hormones including prolactin and oxytocin. During pregnancy there is an increased need for insulin due to the hormones from pregnancy effecting insulin resistance. As the pregnancy advances and the placenta enlarges the need for insulin increases where a latent deficiency can become more apparent.
For the pregnant client the basal metabolic rate increases by 10-20% due to the increased oxygen consumption. The pregnant client must meet their own tissue requirements, fetal growth & development, and prepare for the labor and lactation. The client may also experience increased water retention that is needed for fetal development, placenta, amitotic fluid and blood volume.
