CONTRACEPTIVE COUNSELING
Contraceptive care is primary care. All people with reproductive potential should be counseled about contraception in tandem with reproductive preferences and offered contraception if desired as a part of routine primary care as well as abortion care (Romer 2024). Optimal contraceptive counseling supports all people to make fully-informed decisions based on their stated preferences by providing unbiased, non-coercive information about the range of options (Senderowicz 2020).
Counseling should be responsive to an individual’s priorities and concerns rather than directing them towards using contraception or a specific method or type (Dehlendorf 2014). Preferences vary, but overarching themes include privacy, side effects, safety, bleeding patterns and effectiveness (Ti 2020). Contraceptive counseling must include information on the risks, benefits, and side effects of methods that meet stated preferences. Quality and effectiveness of counseling may be measured by a validated person-centered contraceptive counseling (PCCC) measure (Dehlendorf 2018, 2023).
Unsatisfied preferences have been associated with higher rates of method discontinuation and subsequent pregnancy (Burke 2023). Conversely, outcomes show people are more likely to be satisfied with their counseling, to continue use, and to like a selected method 6 months later if providers use tenets from the PCCC measure.
The PCCC scale focuses on these 4 tenets (from the person’s perspective):
- Respect me as a person
- Let me say what matters to me about my birth control
- Take my preferences about my birth control seriously
- Give me enough information to make the best decision about my birth control method (Dehlendorf 2023)
Core principles / steps in quality contraceptive counseling include:
- Establish and maintain rapport
- Assess preferences, needs, and desires, and personalize discussions accordingly
- If there is a strong interest in one method, ask permission before providing information on others.
- Consider methods that align with personal priorities/preferences, such as:
- Changes to menstrual bleeding
- Route, ease of use or remembering, and cost
- Privacy from a partner or family members
- Effectiveness
- Hormonal or non-hormonal
- Impact on sex and / or pleasure
- Immediacy of effect
- Desire to avoid a foreign object in the body (such as w/ an implant/IUD)
- Work collaboratively to establish a plan
- Anticipate & address barriers to accurate/consistent use for chosen method
- Streamline the decision process (i.e. appropriate language and visual aids)
- Confirm understanding
- Using active learning strategies such as teach back (CDC QFP 2024).
Contraceptive Counseling in the Context of Abortion Care
Offer to discuss contraception, remaining aware that many prefer not to discuss at time of abortion (Brandi 2018, Matulich 2014). If interested, elicit preferences and review options and timing for initiation, noting that all methods can be started the day of procedural abortion, and the majority can be initiated the same day mifepristone is taken, with the exception of IUDs which can be started at follow-up (CDC MEC 2024). Reassure people that abortion does not affect future fertility and that fertility may resume within a week of an abortion.
Counseling For Side Effects And Common Concerns
Many people have fears and opinions about methods based on personal or peer experience (Simmons 2023). Investing in a person’s experience requires authentically listening to and identifying their concerns and preferences.
- Empathize: “That sounds really difficult.”
- Normalize and validate: “I hear that from a lot of people.”
- Offer information and options: “You have options and I’ll support you with any of them. We can wait to see if the symptoms improve, try a treatment to help with the symptoms, or we could stop/remove the method now (or give you information on IUD self-removal).”
- Make a plan: “We can start this method today, but let’s check in in two weeks to discuss any questions or concerns.”
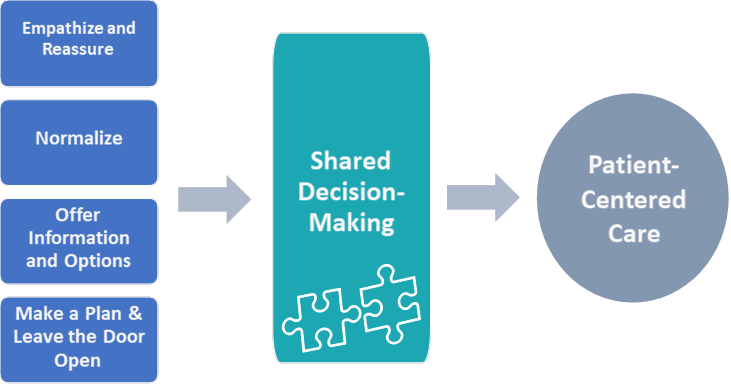
Image from UCSF Beyond the Pill Program