U.S. LAW AND POLICY HIGHLIGHTS
Abstracted from Guttmacher State Bans on Abortion throughout Pregnancy, March 2025
U.S. Abortion Laws After Roe
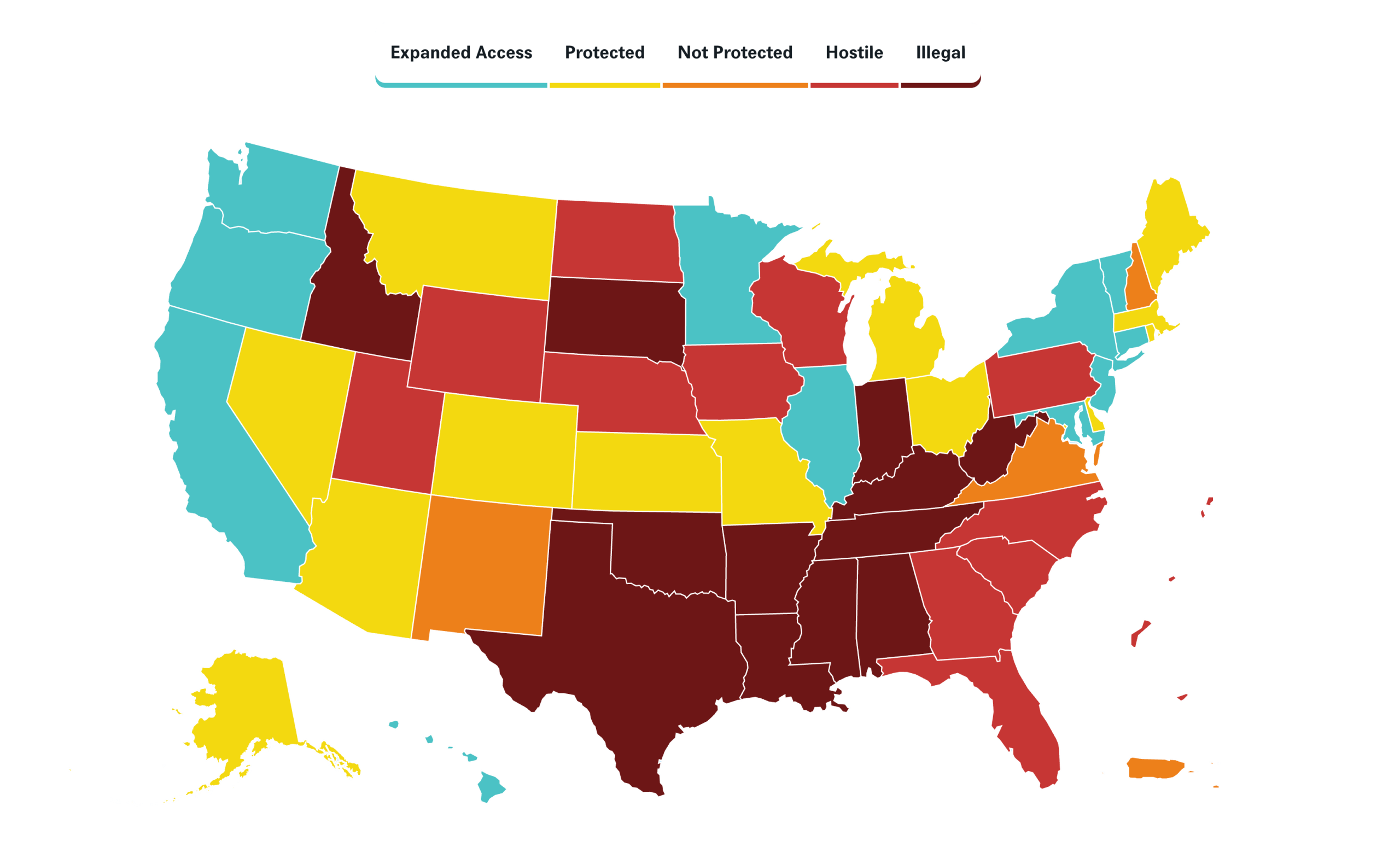
See Center for Reproductive Rights for interactive versions updated in real time (May 2022b).
- Abortion Restrictions and Bans. Abortion provision is completely illegal in 12 states. Additionally, 29 states have abortion bans based on gestational duration, including 7 states at or before 18 weeks’ gestation and 22 at some point after 18 weeks. A total of 9 states and the District of Columbia do not restrict abortion on the basis of gestational duration.
- Note: when discussing abortion as illegal or banned, it is generally the provision or support of someone getting an abortion that is illegal. Thus, the person providing or supporting abortion care is breaking the law. As currently written, the person having the abortion is not breaking the law; including traveling for an abortion.
- Only one state criminalizes ending one’s own pregnancy. Nevada criminalizes any act taken to end a pregnancy after 24 weeks of pregnancy. It is not a crime to use abortion pills to end one’s own pregnancy before 24 weeks in any state.
- People are also criminalized for self-managing abortions and experiencing adverse pregnancy outcomes in the absence of laws permitting such charges (Huss 2023). States have usually used child endangerment laws to prosecute and criminalize people who have an abortion or pregnancy loss (Pregnancy Justice 2024). The majority of pregnancy criminalization takes place in the three states that have case law authorizing use of criminal child endangerment laws to prosecute people who use drugs during pregnancy, post-Dobbs occurred in Alabama, and Oklahoma, and South Carolina. (Pregnancy Justice 2024).
- There are currently no laws requiring health care providers to report people for having an abortion—self-managed or otherwise—to law enforcement, and doing so is a HIPAA violation (IfWhenHow 2024).
- Restrictions, including gestational duration limits, even in states where abortion remains legal, create significant barriers to access and contribute to a complex and often prohibitive environment for individuals seeking abortion services.
- Gestational Duration Limits: 29 states enforce gestational limits on abortion. 4 states limit abortion at 6 weeks, 2 at 12 weeks, 1 at 15 weeks, 1 at 18 weeks, 3 at 22 weeks, 4 at 24 weeks (including Massachusetts, which bases gestation on implantation, effectively making that a 26-week ban), 11 at viability, and 1 at third trimester. Ten states have no gestational duration limit. Most provide exceptions to protect the patient’s life or health (KFF 2024a), although these exceptions often fail in practice due to the environment of fear and legal uncertainty they create (Guttmacher 2025d).
- Public Funding: The Hyde Amendment bars use of federal funds (including military and Indian Health Service funds) to pay for abortion. 20 states utilize their own funds to cover all or most deemed “medically necessary” abortions for Medicaid enrollees. Conversely, 30 states and D.C.restrict state funds, permitting their use only in cases of life endangerment, rape, or incest.
- Private Insurance Coverage: In states where abortion remains legal, 10 states restrict abortion coverage by private insurance plans, often limiting coverage to instances of life endangerment. Some states offer additional abortion coverage at an extra cost.
- State-Mandated Counseling, Waiting Periods, & Multiple Trips: Certain states mandate medically inaccurate counseling, such as the purported link between abortion and breast cancer, fetal pain perception, and long-term mental health consequences (KFF 2024b).These states often also enforce mandatory waiting periods, with many requiring in-person counseling, necessitating individuals make multiple trips to a clinic—an added overall expense and burden for those traveling long distances.
- Medically Unnecessary Ultrasound (US): In several states, laws still require an US, regardless of medical necessity. Some laws also require people seeking care to view and hear US descriptions, even if they object.
- Parental Involvement: Many states require parental consent or notification for minors seeking an abortion. 21 states mandate parental consent and 10 require one or both parents to be notified.
- Targeted Regulation of Abortion Providers (TRAP): TRAP laws impose medically unnecessary restrictions on abortion providers and facilities, such as requiring hospital admitting privileges or compliance with surgical standards, even for clinics that solely provide medication abortion.
- Telehealth MAB Banned: 29 states have laws mandating unnecessary barriers to medication abortion, including 22 states that require an in-person visit and 18 that prohibit telehealth for any abortion service.
- Refusal: Most states where abortion remains legal allow individual healthcare providers and institutions to refuse to participate in an abortion, regardless of whether or not they have a religious affiliation. Beyond abortion, 10 states permit healthcare institutions or providers—including pharmacists—to refuse to provide contraception services, including emergency contraception, disproportionately affecting individuals in restrictive states and rural areas (KFF 2025a).
- Clinician Requirements: Several states have changed their clinician requirements, such that 20 states plus D.C. allow APCs to provide both medication and procedural abortion care. While 2 states allow APCs to provide medication abortion care only (Jenkins 2025).
- Hospital Requirements: 19 states require an abortion to be performed in a hospital after a specified point in the pregnancy, and 17 states require the involvement of a second provider after a specified point.
- Global and Domestic Gag Rule: Prohibits foreign NGOs receiving U.S. global health funding from providing, counseling on, or referring for abortion services. Domestically, Title X-funded clinics cannot use those funds for abortion care or referrals. FQHCs and other federally funded clinics must separate abortion services from federal funds but are not prohibited from provision (See Ch. 10: Addressing FQHC Considerations; RHAP 2024, KFF 2025b).
- Protection Against Clinic Violence: The Freedom of Access to Clinic Entrances (FACE) Act was a 1994 federal law that protected clinics, health care personnel, and people seeking reproductive health care against blockades and violence. While 16 states and D.C. passed similar laws, the current administration has directed federal prosecutors to limit enforcement.
- Federal Abortion Ban: The so-called Partial Birth Abortion Ban Act was upheld in 2007, retreating from an unbroken line of precedent that a patient’s health must be the paramount concern in any abortion regulation, as it includes no health exception. This ban effectively bans the procedure known as dilation and evacuation (Haddad 2009).
- Interstate Shield Laws: Designed to protect abortion providers, those assisting in care, and health records in shield states from enforcement actions by restrictive states. While 23 states and D.C. have some form of shield law, protections vary. Only 8 states explicitly protect providers regardless of the patient’s location, allowing provision of telehealth medication abortion to people in banned states, while others shield providers only when caring for individuals within their state (KFF 2025c). As of the date of publication, their full legal strength is being tested in the courts. These laws play a crucial role in expanding geographical access to abortion care.
Preventing Provider Criminalization
In light of the ever-changing legal landscape of U.S. abortion care, providers and staff should be aware of their constitutional rights when interacting with law enforcement in order to prevent provider and patient criminalization.
- Abortion providers, nurses, and staff have a constitutional right to remain silent and are not required to speak to law enforcement. You cannot legally be punished for refusing to answer police questions.
- Police can legally use deception tactics to obtain information, so it is important to be exceptionally clear when communicating with them (ie, “I will not be answering any questions without speaking to my attorney”).
- Always collect the name and badge number of the officer attempting to communicate with you.
- When speaking with law enforcement, anything you say can be used in a criminal, civil or administrative proceeding against you or potentially someone else, including a patient (ACLU 2025). If you have started to answer questions or provide information to the police, you can stop at any time and consult with an attorney—the ACLU’s Abortion Criminal Defense Initiative and the Abortion Defense Network are good resources for obtaining legal representation.
- Law enforcement are entitled to enter any area open to the public; this usually means police can enter a waiting room. If police request consent to enter other areas of your workplace without a warrant, you have the right to refuse (ACLU 2025).
- Healthcare providers are not required to provide or show law enforcement anything requested without a court order (including health records) (ACLU 2025), and doing so may be a HIPAA or state privacy law violation. If you receive a subpoena, contact your lawyer right away—they may be able to quash the subpoena or limit its scope (ACLU 2025).
- With a search warrant, law enforcement can enter the premises to search for things identified in the warrant. Do not interfere in the search—but ask for a copy of the warrant and contact your attorney. You are not required to tell police where things are located or unlock locked areas or cabinets (ACLU 2025).
Additional Resources: