UNITED STATES ABORTION FACTS AT A GLANCE
Abstracted from Guttmacher Institute’s Abortion in the United States Fact Sheet; 2025c
Abortion By The Numbers
- Abortion is common and much safer than carrying a pregnancy to term, having a colonoscopy, or crossing the street (Raymond 2012, Pedbikeinfo, Levin 2006).
- 21% of U.S. pregnancies (excluding miscarriages) end in abortion (Jones 2022).
- Most abortions occur early in pregnancy; with 93% occurring at < 14 weeks (CDC 2024).
- Medication abortions accounted for nearly two-thirds of all clinician-provided abortion in 2023 (Guttmacher 2025c).
- Telehealth abortion now accounts for 20% of all abortion care (SFP 2024).
- Projected lifetime prevalence of self-managed abortion was estimated at 10% in 2023 (Ralph 2024).
Who Has Abortions
- One of every four U.S. people with pregnancy potential, from all backgrounds, has abortions. Nearly half of these (45%) will have more than one abortion (Guttmacher 2024).
- Approximately 60% of abortions are among people with at least one child.
- 30% identify as Protestant and 24% as Catholic.
- Approximately 60% are in their 20s and 10% are in their teens.
- Approximately 30% identify as White, 29% Black, 30% Hispanic, 4% Asian or Pacific Islander, and 7% different race or ethnicity.
- Approximately 70% of people accessing abortion are low-income or poor.
- Nearly 60% of individuals seeking abortion in abortion-supportive states experience delay-causing obstacles, including cost (45%), geographical access (43%), and travel time (35%) (Wasser 2024). Such delays are compounded for those who live in states without legal access to abortion.
- Transgender and gender diverse (TGD) people may get pregnant before, during, or after transitioning socially, medically, or both, and seek prenatal or abortion care (Moseson 2020).
Long-Term Turnaway Outcomes (ANSIRH TURNAWAY STUDY)
- Long-term research shows that abortion does not harm people; there is no increased risk of depression, PTSD, low life satisfaction, or other mood symptoms when comparing those who had abortion vs. those turned away.
- People denied an abortion have decreased financial security and four times the odds of living below the federal poverty level (FPL) compared to those who had an abortion.
- People denied an abortion are more likely to remain tethered to abusive partners, and to experience pregnancy complications including eclampsia and death.
- The financial wellbeing and development of children is negatively impacted when their parents are denied abortion.
Changes Since Dobbs (SFP #WECOUNT STUDY)
- There has been a consistent increase in both in-person and telehealth abortion volume, and the monthly abortion count increased from 81,400 to ~98,000 abortions between 2022 and the first six months of 2024.
- In most abortion ban states, abortion numbers stayed stable or increased from 2020 to 2023, with most individuals accessing abortion through out-of-state travel or telehealth.
- Telehealth abortion services increased, even in states where abortion remains legal, growing from 4% to 20% of all abortions by June 2024. Both medication abortion and telehealth provision increased during the pandemic and after the Dobbs decision, with demonstrated safety, efficacy and acceptability (Qaderi 2023).
- Following the Dobbs decision, access has been restricted to a broad range of medications with potential to prevent, end or complicate a pregnancy, resulting in delays or denials in receiving prescribed treatments. Examples include access to contraceptive methods to treat medical conditions, methotrexate to treat rheumatoid arthritis or lupus, and antiseizure medications due to teratogenic properties (National Health Law 2024).
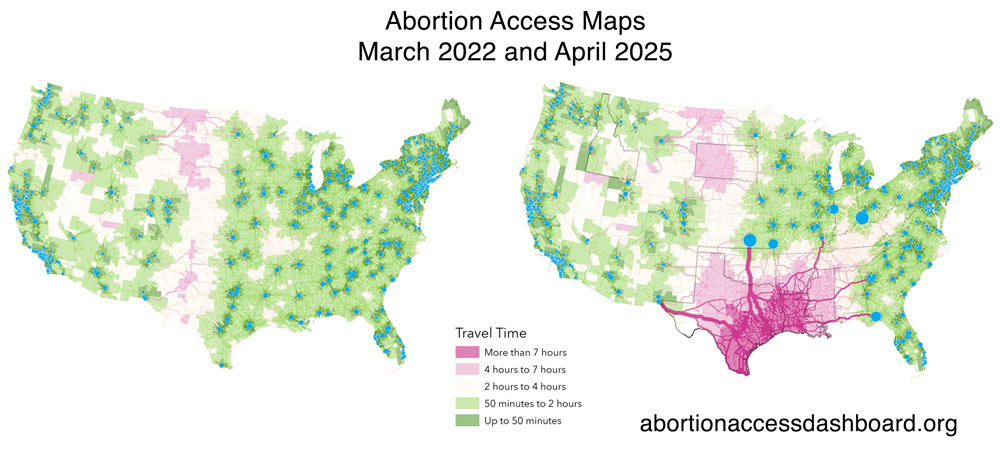
Maps of the contiguous U.S. in March 2022 (pre-Dobbs) and April 2025 showing population-weighted average distance from census tracts to the nearest abortion facility. Source: Myers Facility Database. For interactive maps see the Abortion Access Dashboard (Myers et al. 2025).
Who Provides Abortions
- U.S. abortion providers include obstetrician-gynecologists, family and internal medicine physicians, pediatricians, and advanced practice clinicians, including nurse practitioners, midwives, and physician associates. Many states with current abortion bans and restrictions are the same states that, before Dobbs, had physician-only laws (Sagar 2023).
- At least 40% of providers now offer medication abortion services only (Jones 2024).
- The number of abortion providers and clinics has declined in recent years, even before the Dobbs decision.
- The number of providers decreases with increasing gestational duration: 95% offer abortion to 8 weeks, 34% to 20 weeks, and 16% to 24 weeks (Jones 2019).
- While most states allow healthcare professionals to refuse involvement in abortion based on conscientious objection, many characterize their provision of abortion as conscience-based (Harris 2012). Additionally, professions have specific requirements to ethically exercise conscientious objection, which cannot preclude or unacceptably delay care (Eagen-Torkko 2020).
Contraceptive Use
- Over 50% of people having abortions used a contraceptive method during the month they became pregnant (Jones 2018).
- Of those who did not, 33% perceived themselves to be at low risk for pregnancy, 32% had method concerns, 26% had unexpected sex, and 1% were forced to have sex (Jones 2018).
- 76% of pill users and 49% of condom users reported inconsistent use (Jones 2018).
Safety Of Abortion
- The major report from NASEM (the National Academies of Sciences, Engineering and Medicine) concluded that all forms of abortion (medication, aspiration, dilation and evacuation, and induction) are safe and that the primary factors decreasing safety are those decreasing access (NASEM 2018, Upadhyay 2015, White 2015).
- Having an abortion is over 30 times safer than remaining pregnant, giving birth, and being postpartum in the U.S. (Stevenson 2023). Prior work compared the risk of abortion with the mortality risk of delivery, excluding deaths during pregnancy and postpartum thus understating the risk. As with maternal mortality, Black people have a risk of abortion-related mortality that is 3 times higher than white people (Zane 2015).
- Medication abortion care administered by telehealth and delivered via mail, is feasible, safe, and efficacious (Upadhyay 2021).
- Abortions pose no long-term risk of infertility, ectopic pregnancy, spontaneous abortion, or breast cancer (Guttmacher 2025c), but may increase the risk of subsequent preterm birth (Yu 2023).
- Abortion does not pose a hazard to mental health (Biggs 2016, Horvath 2017). The most common emotional response is a sense of relief (Steinberg 2020).
- The U.S. risk of abortion complications requiring hospitalization is less than 0.5% (NASEM 2018, White 2015).
The Impact Of Abortion-Related Stigma
- People who have had abortions experience fear of social judgment, self-judgment and a need for secrecy. Secrecy was associated with psychological distress and social isolation (Guttmacher 2016).
- Individuals may choose not to disclose their decision to family or friends, to exclude abortion in their health history, or to delay abortion care or management of emergencies.
- Stigma and silence of patients and providers can produce a vicious cycle; “their silence can perpetuate a stereotype that abortion remains rare, or that legitimate, mainstream providers do not perform abortions, contributing to marginalization of patients and providers” (Harris 2013).
- Stigma can lead to the social, medical, and legal marginalization of abortion care around the world and is a barrier to maintaining access to high-quality, safe abortion care.