7 Adhesive Capsulitis
Adhesive capsulitis, also known as frozen shoulder, is a condition in which inflammation within the capsule of the glenohumeral joint leads to its contracture and, with that, significant loss of motion and pain. Primary adhesive capsulitis describes the idiopathic presentation of these symptoms, while secondary adhesive capsulitis appears because of trauma, infection or other medical conditions such as diabetes or hypothyroidism. The painful phase of adhesive capsulitis usually resolves after a period of months, though some residual loss of motion remains even after the pain abates. Histologically, adhesive capsulitis is characterized by fibroblastic proliferation of the coracohumeral ligament and rotator interval, though very few cases progress to the point that a biopsy would be performed. Thus, adhesive capsulitis is usually a diagnosis of exclusion: it is the diagnosis applied to shoulder pain and lost motion where no other cause can be found.
Structure and Function
The glenohumeral joint of the shoulder is a ball and socket joint in which the glenoid cavity of the scapula forms a socket for the humeral head. Unlike the femoral head of hip, the humeral head in the shoulder is not truly constrained within a socket: the glenoid is relatively shallow and thus the relationship of the humerus to the glenoid is akin to that of a golf ball on a tee (See Figure 1). This arrangement allows a far greater range of motion than is seen at the hip – with 120 degrees of unassisted flexion, the glenohumeral joint is the most mobile joint in the body. This motion, though, comes at the price of stability.
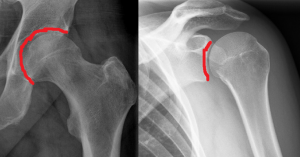
Stability of the glenohumeral joint is provided by the soft tissues. Dynamic (active) stability is a product of paired rotator cuff contraction, which tends to compress the humeral head into the glenoid cavity. The main source of static (passive) stability comes from the joint capsule (Figure 2) and ligaments, with some static stability coming from the glenoid labrum, which effectively deepens the glenoid.

Adhesive capsulitis is caused by contracture of the capsule and intra-articular adhesions which physically tether the joint capsule to surrounding bone and tissues and further limit motion.
Histologically, early adhesive capsulitis is dominated by inflammation of the synovium. With disease progression, the inflamed synovium is replaced with diffuse fibrosis of the shoulder capsule.
Primary adhesive capsulitis is idiopathic. Adhesive capsulitis is also associated with medical conditions (such as diabetes mellitus, thyroid disease and stroke); medical interventions (such as prolonged immobilization, cardiac surgery and antiretroviral therapy for HIV); and injuries (such as rotator cuff tears or proximal humerus fractures). When there is an associated cause, the condition is designated as secondary adhesive capsulitis.
Patient Presentation
The hallmarks of adhesive capsulitis are pain and decreased motion. Needless to say, there are many conditions which cause either pain or decreased motion or both; adhesive capsulitis can appear as an isolated condition or accompanying another shoulder condition.
Patients with adhesive capsulitis present with gradual unilateral shoulder pain that is often diffuse and worse at night. They also report an insidious onset of increasing stiffness. Some patients may “remember” a trivial trauma inciting the process, though this is likely a faulty attribution.
Clinically, isolated adhesive capsulitis has 3 distinct phases, namely: the painful phase, the stiff phase, and the resolution phases.
The Painful (or “freezing”) Phase begins gradually, with no known precipitant. This phase, which lasts weeks to months, is characterized by diffuse, disabling pain that is worse at night.
The Stiff Phase is noted by marked stiffness that limits range of motion in multiple planes, interfering with activities of daily living. Pain is less intense at this point. This phase can last a year or longer.
Most patients enter a Resolution (“thawing”) Phase during which motion improves, though often some limitations of range of motion compared to the contralateral shoulder remain.
On physical exam, patients with adhesive capsulitis have significantly reduced active and passive range of motion in two or more planes (see Figure 3 for normal ranges of motion). External rotation and abduction are the most commonly affected movements. Patients also have difficulty internally rotating. They might report problems scratching their back, for example, or hooking their bra from behind.

The critical finding of adhesive capsulitis is a loss of the end range of passive shoulder motion that is not limited by either pain or an intra-articular blockage. Adhesive capsulitis is a clinical diagnosis, made once radiographic evidence of underlying rotator cuff pathology and osteoarthritis is excluded. An inconsistent range of lost motion on examination precludes making the diagnosis of adhesive capsulitis. Lost motion of an inconsistent degree is more likely due to pain, malingering or other forms of active limitation, and not capsular contracture.
An intra-articular injection of an anesthetic can help eliminate the restrictions of motion imposed by pain.
Objective Evidence
Radiologic imaging does not diagnose adhesive capsulitis, but clinicians will often obtain plain radiographs to asses for glenohumeral arthritis or other shoulder pathologies. Plain radiography is usually normal in adhesive capsulitis.
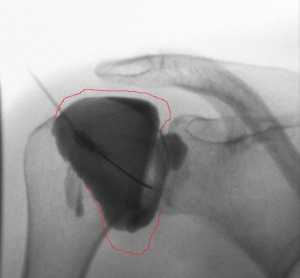
Arthrography, in which the contracted joint is injected with contrast prior to imaging, can reliably diagnose capsular contracture: the normal shoulder accepts 20 ml of fluid without difficulty, but with adhesive capsulitis the shoulder usually holds less than 10 ml (Figure 4). Nonetheless, the degree of lost volume does not correlate perfectly with the degree of lost motion.
In primary adhesive capsulitis, there are no specific laboratory findings. Nonetheless, lab tests are commonly obtained once the diagnosis is made, to help identify a cause (e.g., diabetes).
Ultrasound can be used to rule out rotator cuff or bursal pathology. On ultrasound, thickening of the coracohumeral ligament and increased vascularity around the intraarticular portion of the biceps tendon may be seen with adhesive capsulitis.
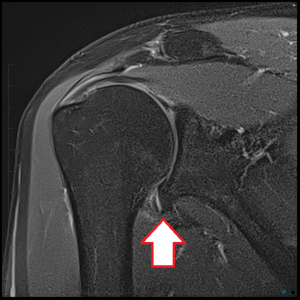
Magnetic Resonance Imaging is also used to investigate the painful shoulder, as it is very sensitive for rotator cuff disease. MRI findings in adhesive capsulitis include thickening of the coracohumeral ligament and joint capsule with associated edema at the rotator cuff interval. MRI may demonstrate capsular thickening and decreased axillary pouch filling (Figure 5).
Epidemiology
It is estimated that approximately 5% of the general population, and 20% of patients with diabetes, will develop adhesive capsulitis in their lifetime. Adhesive capsulitis typically affects patients in their fifth or sixth decade, with a predilection for women. The non-dominant side is more frequently affected, though this bias may be a function of the patient’s ability to not use the non-dominant side, which thereby allows the soft tissues to stiffen. Symptoms will develop in the contralateral shoulder in approximately 20% of cases.
Differential Diagnosis
The initial painful phase of adhesive capsulitis can overlap with subacromial bursitis/rotator cuff tendinopathy. Isolated adhesive capsulitis is usually not associated with repetitive motion or specific overhead activities. Also, adhesive capsulitis on physical exam is characterized by stiffness in more than one plane of motion. Adhesive capsulitis causes lost passive motion, whereas in cuff disease the range of passive motion is normal (though painful).
Another aspect of the patient history that can be very helpful in differentiating between different pathologies is the patients age. Primary adhesive capsulitis is rare in patients younger than 40 or older than 70 years.
Lost motion can be caused by glenohumeral arthritis, and therefore the diagnosis of adhesive capsulitis is reserved for cases in which no significant degenerative joint disease is seen.
The pain of adhesive capsulitis is usually found at the endpoint of motion, as the capsule is stretched. Until that is encountered, symptoms are minimal.
Sudden loss of motion may be caused by an unrecognized dislocation.
Other notable diagnoses to consider are neck pathology, cervical spine degeneration, diaphragmatic irritation, myocardial ischemia especially in an elderly female, or apical lung malignancy.
Red Flags
Night pain that awakens the patient from sleep may be due to occult malignancy that requires accurate diagnosis to guide treatment. Chronic shoulder pain with radiculopathy may suggest cervical spine pathology.
Treatment Options and Outcomes
Adhesive capsulitis is a self-limiting disease, yet benign neglect is usually poorly tolerated. Due to the protracted course of adhesive capsulitis, which can take 2 years to resolve, many patients are unsatisfied with this lengthy period of pain and disability and are not comforted by the knowledge that the condition will eventually resolve. The pressure to “do something” is great.
The most commonly employed treatment for adhesive capsulitis is physical therapy to prevent soft-tissue contracture as well as to improve shoulder motion. This treatment may be limited to passive motion, as the patient is too symptomatic to do more actively.
Pharmacologic intervention is often included as empiric treatment in conjunction with therapy. Oral non-steroidal anti-inflammatory drugs may be given to modulate shoulder pain (whether they decrease capsule inflammation is not known).
Patients may also receive intra-articular corticosteroid injections for pain relief. The benefits of oral corticosteroids have not been shown to outweigh their risks. Intra-articular steroid injections may better optimize local concentrations of medicine and avoid systemic effects. Adding a large volume of saline may help lyse adhesions and stretch the capsule (a procedure known as “infiltration brisement” or “hydro-dilution”). This has a risk of capsular rupture, however.
Manipulation under anesthesia is generally regarded as a second-line treatment, chosen when non-operative treatments fail. Some potential risks include iatrogenic humeral dislocation or fracture, and soft tissue injury such as rotator cuff or labral tears.
Arthroscopic capsular release may be chosen in severe cases. Arthroscopic treatment has several advantages including visualization and exclusion of other diagnoses and focal lysis of adhesions in the coracohumeral ligament, rotator interval and inferior pouch (unlike manipulation, which stretches everything indiscriminately). Additionally, active range of motion can be performed soon after surgery to prevent new scar formation. Despite its advantages, arthroscopic capsular release is not without risks. Entering the joint capsule can be difficult due to a thick capsule and reduced joint space making insertion of trocars difficult and potentially damaging to the articular cartilage if excess force is applied.
The capsular changes in adhesive capsulitis shares some similarities to the fibrous contractures seen in Dupuytren’s disease. The 2016 Richard A. Brand Award winning paper reported promising results using collagenase, an enzyme used in the treatment of Dupuytren’s, to treat adhesive capsulitis.
Although adhesive capsulitis is a self-limiting disease, some patients may continue to demonstrate either shoulder pain and/or stiffness at 7-year follow-up.
Despite widespread use of physical therapy for the treatment of adhesive capsulitis, little evidence supports its use: a Cochrane database review was unable to confirm its benefit as a treatment. Still, retrospective case series evidence has demonstrated 90% of patients treated with a multi-directional stretching program were satisfied with their clinical result and given the pressure to take some action, this approach seems justified even in the face of poor evidence.
Treatment with oral medication has no high-level evidence supporting its use for treatment of adhesive capsulitis. One study has demonstrated that a 4-week regimen of naproxen or indomethacin had similar success for lowering pain levels. Risks of NSAID use include GI distress.
Risk Factors and Prevention
Secondary adhesive capsulitis is associated with medical conditions such as diabetes mellitus, thyroid disease and stroke; medical interventions such as prolonged immobilization, cardiac surgery and antiretroviral therapy for HIV; and injuries such as rotator cuff tears or proximal humerus fractures.
Prevention of adhesive capsulitis centers on maintaining motion after an event of diagnosis that is associated with secondary adhesive capsulitis. Early shoulder mobilization after surgery is especially helpful for the retention of motion.
Miscellany
EA Codman coined the name Frozen Shoulder in 1934
Keywords
adhesive capsulitis, capsule
Skills
Recognize adhesive capsulitis and distinguish it clinically by history and physical exam from other common shoulder pathologies. Describe treatment options for the management of adhesive capsulitis along with their risks and benefits.
