6 Disorders of the Rotator Cuff
The rotator cuff comprises four muscles that originate on the scapula and insert on the humerus: the supraspinatus, infraspinatus, teres minor and subscapularis. Although these muscles have distinct effects on the humerus (often overlapping with non-rotator cuff muscles), the collective effect of the rotator cuff is to dynamically constrain the humeral head. Rotator cuff tears may be sudden and traumatic or gradual and attritional over time. Treatment ranges from benign neglect to surgical repair, depending on the functional loss of the injury and the patient’s functional needs.
Structure and Function
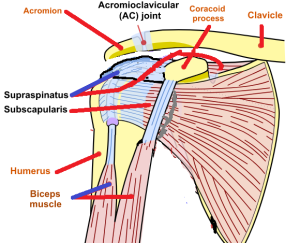
The rotator cuff is the collective term for the four muscles that originate on the scapula and insert on the humerus: the supraspinatus, infraspinatus, teres minor and subscapularis. Because their insertion is (somewhat) confluent, they are collectively designated a “cuff” (Figures 1 and 2).
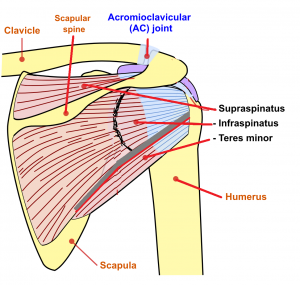
The supraspinatus originates in the supraspinatus fossa on the posterior scapula, crosses the superior humeral head, and inserts on the greater tuberosity.
The infraspinatus and teres minor originate in the infraspinatus fossa on the posterior scapula and insert on the greater tuberosity as well, posterior to the insertion point of the supraspinatus.
The subscapularis originates on the anterior aspect of the scapula and inserts on the lesser tuberosity.
The primary purpose of this cuff is to constrain the humeral head and initiate abduction and elevation. Recall that the glenoid is fairly shallow and that the shoulder is not a true ball and socket joint. If there was no constraint on the humeral head, the pull of the deltoid muscle, for example, will simply move the humeral head in a rostral direction. The rotator cuff primarily stabilizes the shoulder by compressing the humerus into the glenoid fossa. If the rotator cuff is able to constrain the humerus, a fulcrum is created, and the deltoid will then elevate or abduct the arm.
Additionally, the muscles of the rotator cuff can move the humerus: the supraspinatus produces abduction in the scapular plane; the infraspinatus and teres minor provide humeral external rotation; and the subscapularis produces internal rotation. Note that there is redundancy with other non-cuff muscles such that a rotator cuff tear – especially one developing chronically, over time – does not necessarily create a functional loss.
Complicating matters, it is possible to have overlapping diagnoses (some rotator cuff disorder coupled with some arthritis, for example), and it is possible to have anatomic abnormalities of the rotator cuff that are simply not responsible for the patient’s symptoms – at least to the extent that fixing the anatomic abnormality may not make the patient better. This latter consideration is especially important given the recognition that highly sensitive testing modalities such as MRI are almost certain to detect abnormalities in people middle-aged and older, and it would be wrong to pounce upon an anatomic finding as a necessary explanation for a patient’s pain.
Patient Presentation
Patients with symptomatic rotator cuff disorders typically report pain in the anterior or lateral shoulder (greater tuberosity), especially with overhead activity.
There may be a prodrome of mild symptoms, with a superimposed worsening after an acute event.
On exam, patients might demonstrate weakness and pain with arm movement in the affected tendon’s plane of motion. Because of the great redundancy of muscles coursing from the scapula or torso to the arm, some patients may have a so-called compensated rotator cuff tear, and have no functional loss despite losing the function of one or more rotator cuff tendons.
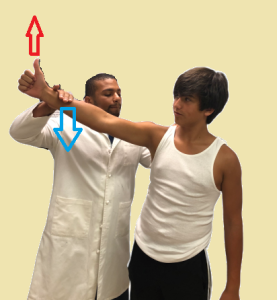
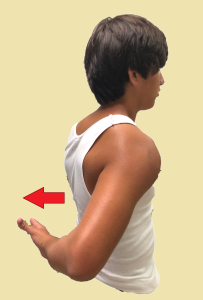
The physical examination should measure active and passive motion in elevation, abduction, and internal and external rotation. Specific maneuvers are shown in Figures 3 to 6.


Loss of the bulk of the rotator cuff muscles on the posterior aspect of the scapula may suggest a chronic tear.
Objective Evidence
Plain radiographs are helpful in detecting arthrosis, calcific deposits in the tendons, and bone spurs. Large and long-standing cuff tears may also result in proximal humeral head migration relative to the glenoid.
Ultrasound is said to be both sensitive and specific for the identification of rotator cuff tears but is highly operator dependent.
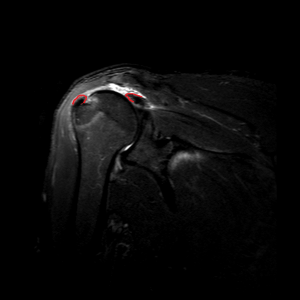
Magnetic Residence Imaging (MRI) is also thought to be sensitive for the identification of rotator cuff tears (Figure 7). This modality is particularly useful for measuring the size of any tear, if present, and the presence or absence of tendon retraction, and muscle atrophy. The problem with MRI is that it may be too sensitive and can show things that are not necessarily clinically significant. In particular, MRI can detect a so-called partial thickness tear, in which the insertion of the muscle tendon unit is preserved however there is intrinsic damage to the tendon in its course. (The phrase “partial thickness tear” uses the word “tear” as it would be used in the phrase “wear and tear”.) The relationship between this finding and the patient’s symptoms is not assured.
*
Epidemiology
The majority of rotator cuff tears occur secondary to age related degenerative changes in rotator cuff tissue. As a general rule, a patient of X years of age will have an X% chance of having at least a partial rotator cuff tear on MRI, even if he or she has neither signs nor symptoms. Thus a “positive” test may not point to a meaningful diagnosis.
Rotator cuff tears in young adults are uncommon, but may occur following traumatic injuries, such as a fall on an outstretched arm.
Differential Diagnosis
Dysfunction of a rotator cuff muscle is usually indicative of a tear of that muscle-tendon unit, however a compressive neuropathy (of the suprascapular nerve) may mimic the functional loss of a complete rotator cuff tear.
The differential diagnosis for the symptoms overlapping with rotator cuff disorders includes subacromial bursitis, biceps tendonitis, labral disorders, adhesive capsulitis, glenohumeral or acromioclavicular arthritis, cervical radiculopathy, and shoulder instability.
Subacromial bursitis, also known as “impingement syndrome”, is caused by inflammation of the bursa above rotator cuff tendons, mainly the supraspinatus. It can present with or without tendinopathy on MRI. This presentation was called “impingement” because it was thought to be caused by pressure from the acromion, though that is a misnomer: as noted politely in a leading journal, that theory has not withstood the test of time, based on studies that have shown similar outcomes independent of the presence of bony impingement on the cuff.
Rotator cuff dysfunction suggestive of a complete tear may be manifest even if the tendon is in continuity because of pain. This can be clarified by examination before and after an injection of an anesthetic (e.g., lidocaine) in the subacromial space. If after injection the patient no longer demonstrates weakness, preservation of the tendons’ insertion can be inferred.
Bicep tendonitis may present as a rotator cuff disorder. (The long head of the bicep functions like a fifth rotator cuff tendon, one might say.) Bicep tendonitis can be differentiated on examination by producing pain with elbow motion against resistance.
Adhesive capsulitis (frozen shoulder) might present with signs and symptoms suggestive of rotator cuff disorder, but in this condition passive motion is limited as well.
Motion may also be limited with glenohumeral osteoarthritis. This condition is detected on imaging.
Cervical radiculopathy, especially involving the fifth cervical level, can cause shoulder or arm pain with muscle weakness. In this condition, however, there is usually also decreased sensation or paresthesias, and changes in symptoms with head and neck motion.
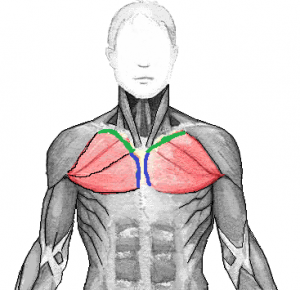
In young male athletes (especially weightlifters), the diagnosis of a pectoralis major (Figure 8) muscle or tendon tear should be considered. Pectoralis major tears typically occur during eccentric contractions, e.g., decelerating the bar in a bench press. Rupture can involve a tear of the muscle belly or tendon, or it can avulse off its insertion on the humerus. After the pectoralis major is ruptured, the patient will have limited horizontal adduction and internal rotation. Patients will demonstrate weakness with adduction and internal rotation, often with ecchymosis on the medial anterior aspect of the arm.
Red Flags
Neurological red flags include sensory deficits, winged scapula, or abnormal reflexes.
Left shoulder pain may have a cardiac origin.
Treatment Options and Outcomes
Patients with rotator cuff disorders should be segregated into those who have had acute deterioration (notably, a sudden inability to elevate the arm) after trauma and those who are suffering from a more chronic pain-related condition. A patient who was highly functional, sustained an injury and had an abrupt loss of rotator cuff function is indicated for surgical repair– once imaging studies confirm the diagnosis, and that the remaining anatomy is amenable to repair. This repair should be performed expeditiously (within a month or so of injury), to prevent retraction of the tendon.
Tears of the pectoralis major should also be fixed, if possible.
Patients who have retained function but are limited by pain may do well with non-operative treatment. It is critical to avoid immobilization of the shoulder during recuperation as that will likely induce stiffness.
Physical therapy focuses on stretching of the posterior and anterior joint capsule, improving scapulohumeral coordination and strengthening the uninvolved rotator cuff. For example, if there is supraspinatus pathology, internal and external rotation exercises can be employed; the rationale of such a strengthening program is that a stronger infraspinatus and subscapularis may be adequate to contain the humeral head, allowing the supraspinatus to rest.
Subacromial injections may provide symptomatic relief. Because steroids are thought to weaken the tendon, by convention no more than a few of these injections are ever given.
Surgical repairs can be performed arthroscopically (Figure 9) or through an open procedure. The torn tendon is identified, debrided and anchored to the humerus (and if possible, sutured to the adjacent tendons as well).

Most patients with rotator cuff disorders improve. It is not clear if this is necessarily from the intervention or the natural waxing and waning of the underlying disease.
Most patients who have surgery also do well, though interestingly outcomes after rotator cuff repair are somewhat independent of whether the tendon actually heals to bone: some patients do well even though the repair does not “take”, whereas others with an intact tendon on postoperative imaging may have persistent symptoms.
(It is known that neglected tendon tears can lead to degenerative arthritis in the glenohumeral joint and that patients who immobilize their shoulders during painful flares can get stiff, bolstering our confidence that interventions are helpful, though it is certainly possible that some clinical improvement after treatment merely reflects the natural history of the disease.)
Patients with work-related injuries and those with ongoing litigation have poor outcomes.
Risk Factors and Prevention
Risk factors for rotator cuff tears include increasing age, repetitive overhead activities and smoking. It has not been proven, but it makes intuitive sense to believe that maintaining the strength of all of the shoulder muscles will prevent dysfunction even if a given muscle were to degenerate or tear.
Miscellany
Mnemonic: The rotator cuff “sits” on the proximal humerus, and thus the names of the four muscles can be remembered by the four letters S I T S. The order of the tendon insertions also follows this mnemonic, coursing around the humeral head starting with the supraspinatus at the 12 o’clock position.
Key Terms
Rotator cuff, degeneration, tears, impingement, tendon repair
Skills
Complete upper extremity musculoskeletal exam and specific shoulder special tests. Interpret radiographs and MRIs for osseous lesions and soft tissue pathology. Demonstrate rotator cuff strengthening exercises to patients.
