9 Glenohumeral Instability
Glenohumeral instability is defined as an inability to maintain the humeral head centered in the glenoid fossa. This problem is typically caused by either a traumatic rupture of the capsule and ligaments (usually following a complete dislocation or partial dislocation/subluxation), or by generalized laxity of the soft tissue. In the case of post-dislocation instability, the shoulder is unstable in only one plane (namely, in the direction of the dislocation), whereas with generalized laxity, the instability is multidirectional. Patients with glenohumeral instability may suffer repeat episodes of subluxation in which the joint surfaces are damaged. In very broad terms, instability from trauma is amenable to surgical repair, whereas multidirectional is not. Multidirectional instability is treated with physical therapy to strengthen the rotator cuff, but this does not always stabilize the joint sufficiently.
Structure and Function
Unlike the femoroacetabular joint of the hip and humeroulnar joint at the elbow, the glenohumeral joint has little static stability provided by the bony anatomy. The humeral head is not constrained by the (relatively shallow) glenoid fossa; rather, only a small portion of the humeral head articulates with the glenoid (Figure 1).
Accordingly, the shoulder relies on both dynamic (active) and static (passive) soft-tissue stabilizers. The main static stabilizers of the shoulder are the ligaments and capsular tissue. Some additional static stability is provided by the labrum, a lip of cartilage around the glenoid that deepens the socket.
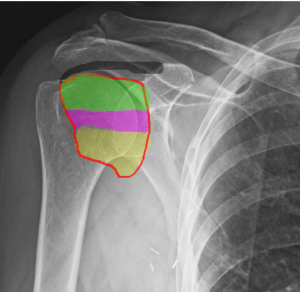
There are regions of the capsule which are identified as distinct ligaments (Figure 2). The superior glenohumeral ligament provides stability with the arm at the side, the middle glenohumeral provides restraint with the arm partially abducted and the inferior glenohumeral ligament is the primary stabilizer with the arm fully abducted.
The rotator cuff, along with the long head of the biceps, stabilizes the glenohumeral joint actively (Figure 3). Paired contraction of the rotator cuff muscles holds the humeral head in close approximation to the glenoid cavity.

The axillary nerve is often injured with shoulder dislocations. The axillary nerve wraps around the surgical neck of the humerus and runs below the humeral head.
Patient Presentation
A thorough history is essential to characterize a patient’s shoulder instability. The patient may recall a specific traumatic instability event. Alternatively, the patient may have numerous incomplete instability events or describe generalized laxity of both shoulders or other joints.
Anterior instability often follows an injury to the arm when it is abducted and externally rotated. In contrast, posterior instability is often caused by a force applied to the arm when it is adducted, flexed and internally rotated. Inferior instability is associated with a history of instability with carrying heavy loads. Although anterior instability is the most common form, inferior, posterior and multidirectional instability must be considered.
With an acute anterior shoulder dislocation, the patient typically presents with the arm held closely at the side. Any attempt to abduct or rotate the arm is resisted because of pain. There is loss of the normal contour of the deltoid. The humeral head itself may be seen or felt anterior to its normal position.
The acute presentation of posterior shoulder instability is more subtle. A lack of external rotation compared to the contralateral normal shoulder may be the only presenting sign.
The physical exam should begin with evaluation of the asymptomatic shoulder for comparison.
Two simple tests may be used even by inexperienced examiners to evaluate shoulder instability.
The sulcus sign can be elicited by applying longitudinal inferior traction of the humerus; that is, by pulling down on the patient’s wrist with the arm held at the side. Excessive inferior displacement of the humerus relative to the lateral border of the acromion creates a sulcus and reflects laxity of the capsule, (Figure 4).

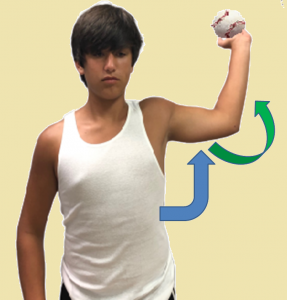
The anterior apprehension test is performed by asking the patient to abduct the shoulder (blue arrow) and externally rotate the arm (green curved arrow) – as if cocking the arm to throw a ball. A patient with anterior instability will be apprehensive in this position or might simply refuse to perform this maneuver (Figure 5).
More subtle anterior instability can be detected by having the supine patient abduct the shoulder and externally rotate the arm, and the examiner can then push on the arm as if to glide the humeral head out of the joint.
Signs of generalized ligamentous laxity include the ability to touch the palms to the floor while bending at the waist; hyperextension of the elbows, metacarpophalangeal or knee joints; and the ability to abduct the thumb to the forearm. The presence of these so-called Beighton criteria is indicative of laxity.
Objective Evidence
To assess patients with suspected shoulder instability, obtain both an anteroposterior (AP) view (Figure 6) and an axillary lateral view of the shoulder. It is important to obtain two orthogonal views. A dislocated shoulder might look normal on the AP view and a dislocation may be missed if only this view is obtained.

Magnetic resonance imaging (MRI) can be used to visualize the ligaments that might be torn with shoulder dislocation (Figure 7). MRI is more sensitive for the detection of labral injury if a contrast medium such as gadolinium is injected into the joint. MRI is especially useful for the evaluation of older patients with a dislocation as they are more likely to have torn the rotator cuff concurrently.

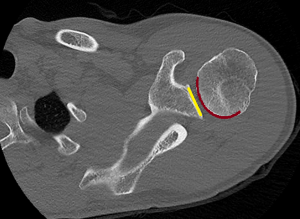
CT scans may be helpful for evaluation of the bony anatomy and should be obtained if there is suspicion of a large Hill-Sachs lesion or glenoid fracture.
Epidemiology
The annual incidence of shoulder dislocations in the United States is approximately 24 per 100,000 people. The incidence rates in military personnel and athletes are considerably higher. Anterior shoulder dislocations account for more than 95% of shoulder dislocations. Posterior dislocations account for about 4%, and inferior shoulder dislocations represent the remaining 1%.
Multidirectional shoulder instability is frequently bilateral. Its incidence peaks in young adulthood (approximately late teens) and is found especially in overhead athletes (pitchers, swimmers and gymnasts) or people with connective tissue disorders such as Ehlers-Danlos or Marfan’s syndrome.
Differential Diagnosis
When patients present with suggested glenohumeral instability, physicians must exclude the following concomitant conditions:
- A Bankart lesion (avulsion of the anterior labrum),
- A “bony Bankart” lesion (a fracture of the anterior glenoid),
- A Hill Sachs defect (impaction fracture of the humeral head, caused by contact against the glenoid during dislocation),
- Fracture of the greater tuberosity (especially in older patients),
- Fracture of the lesser tuberosity (with posterior dislocation),
- Nerve injuries, especially axillary nerve,
- Generalized ligamentous laxity.
Red Flags
Seizures and electrocution can cause posterior shoulder dislocations and should be considered in any patients with that history and shoulder complaints. Likewise, the presence of a posterior shoulder dislocation raises the suspicion of an unreported seizure. Posterior shoulder dislocations are also associated with small lesser tuberosity fractures. These fractures might be missed if the films are not examined closely.
Multidirectional shoulder instability may suggest a connective tissue disorder such as Ehlers-Danlos or Marfan’s syndrome.
Abnormal passive motion suggests that the shoulder is not reduced.
In patients older than 40 years, the orthopaedic surgeon should have a high index of suspicion for a concomitant rotator cuff tear.
Although axillary nerve injuries are seen in only a small minority of cases, they are frequent enough (~5% of cases) that the presence of dislocation itself is a “red flag” for a nerve injury and must be excluded on exam.
Treatment Options and Outcomes
Acute shoulder dislocations should be reduced expeditiously. Any of a variety of reduction techniques can be performed. The Hippocratic method for anterior dislocations uses gentle longitudinal traction applied with a counterforce (e.g., a sheet placed in the patient’s axilla). The Milch maneuver has the patient lying prone on the exam table with both abduction and external rotation forces applied to the arm as the physician’s thumb attempts to push the humeral head into place.
Reduction is easiest when there is full relaxation of the shoulder musculature. Therefore, all attempts at reduction are best supplemented with either conscious sedation or an intra-articular anesthetic injection.
Radiographs after the procedure are required to verify reduction.
After reduction, a short period of immobilization is reasonable, followed by range of motion exercises and then a strengthening program.
Physical therapy alone may be adequate treatment for traumatic instability. Surgery may be considered especially in younger patients with a Bankart lesion or patients with a history of recurrent dislocations. Surgery is typically a repair of the capsule, along with a “shift” to tighten the tissue.
Patients with a shoulder dislocation are considered cleared to play when strength and full range of motion have returned to normal.
Multidirectional shoulder instability is treated with physical therapy – and then more physical therapy if that does not work. Operative stabilization is indicated only if instability that interferes with critical activities persists after extensive non-operative management.
Surgery for multidirectional shoulder instability attempts to plicate (that is, fold over and thereby tighten) the redundant capsular tissue. It is key that this plication is balanced, as too much tightening on one side (anteriorly, say) will just create more instability in the other direction.
The natural history of initial shoulder dislocations remains controversial. Recurrent dislocation is most strongly predicted by the age of the patient. In athletes younger than 20 years of age treated non-operatively, recurrence rates above 50% have been reported. Recurrent dislocation is less common in older patients, but in this cohort rotator cuff tears are more common and surgery may be needed to treat that aspect of the injury.
Athletes who have had a shoulder stabilization procedure after traumatic dislocation report a far lower dislocation recurrence rate (less than 15%) than would be expected from non-operative treatment. Most patients also report excellent subjective and objective clinical outcome scores.
Risk Factors and Prevention
Patients might be at increased risk for shoulder instability for reasons under one’s control (choice of sports, for example) or for reasons beyond individual control (abnormal glenoid anatomy and ligamentous laxity, to name two).
Even if there are non-modifiable risk factors, the odds of a dislocation may be minimized by assuring adequate strength of all muscles crossing the shoulder (including scapular-stabilizing muscles) and by keeping repetitive shoulder stress to a minimum.
Miscellany
Hippocrates not only invented a method of reducing the shoulder (Figure 8), he also devised a means of repairing the tissue injured by dislocation: namely, burning the capsule with a hot poker placed in the axilla. This method is frowned upon by modern authorities.

Key Terms
Glenohumeral instability, anterior dislocation, posterior dislocation, inferior dislocation, subluxation, humeral head, labrum, Bankart lesion, Hill-Sachs defect
Skills
Recognize history and signs suggesting dislocation. Recognize dislocation on imaging, and in particular, whether imaging is inadequate.
