16 Labral Tears of the Hip and Femoroacetabular Impingement
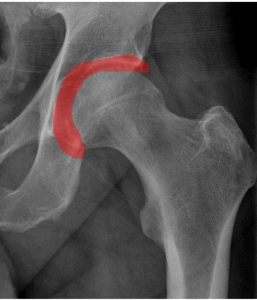
The acetabular labrum is a rim of cartilage surrounding the socket of the hip joint. Damage to the labrum can result from various causes, including trauma and degeneration. Labral tears can be painful, but also may be found incidentally on imaging studies. Femoroacetabular impingement is a clinical syndrome associated with labral tears. This syndrome is characterized by bony overgrowth of either the femur, the pelvis or both (Figure 1). These morphological abnormalities are thought to produce (or at least reflect) abnormal contact between the proximal femur and acetabulum during hip flexion and rotation. It has been proposed that this contact damages the labrum as well as the articular cartilage of the hip joint itself.

Structure and Function
The labrum is a fibrocartilaginous structure surrounding the rim of the acetabulum (Figure 2). In cross section, the labrum is triangular with an articular and capsular surface. The labrum rim functions to deepen the acetabulum, increasing the contact area of the hip joint and thereby reducing cartilage contact pressure and increasing hip stability.
Trauma is a common cause of labral tears. Usually, this involves a mechanism which results in forceful resistance of hip flexion (e.g. tackled while kicking or running).
Hip dysplasia and capsular laxity are associated with labral tears, likely by exposing the labrum to abnormal forces.
Femoroacetabular impingement anatomy is also associated with labral tears. It is important to distinguish between “femoroacetabular impingement anatomy” –that is, the anatomic morphological deviance from normal– and the clinical syndrome of femoroacetabular impingement, which is the combination of the characteristic anatomy and clinical symptoms. Many people have femoroacetabular impingement anatomy without symptoms.
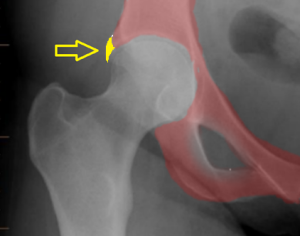
Femoroacetabular impingement anatomy is broadly defined by bony overgrowth of the femur at the femoral head-neck junction, termed “Cam impingement” (Figure 3), or overgrowth of the acetabular rim, termed “Pincer impingement” (Figure 4). Both Cam and Pincer impingement may be found concurrently.
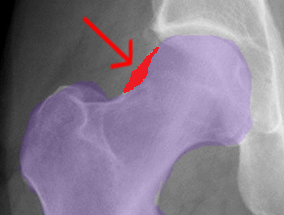
Cam impingement is characterized by a non-spherical femoral head and decreased head-neck offset. During hip flexion, the aspherical femoral head can make contact that shears the acetabular cartilage and the labrum. Labral damage in Cam deformity most often occurs anterosuperiorly, at the transition zone where the labrum blends into the hyaline cartilage.
Pincer impingement is due to acetabular overgrowth and “over-coverage” of the femur. Abnormal contact between the overgrown acetabular rim and femoral head-neck junction leads to tears within the substance of the labrum. Pincer-associated labral tears are also most often in the anterosuperior quadrant of the labrum, though a so-called contrecoup cartilage lesion in the posteroinferior acetabulum may be found as well.
Patient Presentation
Patients with labral tears may present with hip pain and may note clicking, locking, and popping as well. In almost all patients, the pain is located in the anterior hip or groin.
Patients may make a “C sign” – grasping the affected hip with their hand indicating both anterior and posterior hip pain (Figure 5).

On physical exam, flexion, adduction, and internal rotation (Figure 6) can provoke the symptoms of an anterior-superior tear whereas abduction and external rotation (Figure 7) tend to elicit pain in those with posterior labral tears.
 |
 |
Figure 6: Patients with an anterior-superior labral tear will report pain if the examiner passively flexes (red arrow), slightly adducts (white arrow) and internally rotates (green arrow) the hip. |
Figure 7: Patients with posterior labral tears will report pain if the examiner abducts (white arrow) and externally rotates (green arrow) the hip. |
These tests are performed when the patient is supine and the hip and knee are flexed to 90 degrees.
Hip range of motion may be limited, especially in rotation, but this is not a specific finding.
Objective Evidence
MRI is the most sensitive method of imaging and study of choice to evaluate for chondral or labral damage (Figure 8).
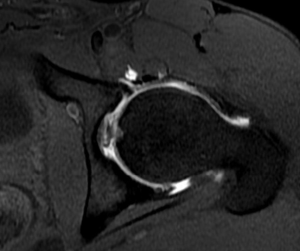
Nonetheless, MRI may miss clinically significant findings. MRI arthrogram (MRI with contrast material injected into the joint), is the study of choice to identify labral tears.
CT scans help better characterize the bony deformities in femoroacetabular impingement and assist in surgical planning.
Most patients with labral tears (85% or more) have some radiographic abnormality. That is to say, labral tears are rarely found in hips with normal bony anatomy. Thus, while normalcy does not exclude the diagnosis, it makes it less likely.
(Note that the finding that most patients with labral tears have some radiographic abnormality does not mean that these abnormalities cause the tear. For one thing, there may be many people with these abnormalities that do not have a tear. The other possibility is that the radiographic abnormality, e.g. bone overgrowth, is caused by the labral tear, and not the other way around.)
Initial radiographic evaluation of patients with symptoms concerning for femoroacetabular impingement or labral pathology should be an anterior posterior pelvis and lateral hip film. Frog leg or cross table lateral may also be used. However, a 45 degrees Dunn lateral (hip flexed to 45 degrees and abducted 20 degrees) provides the most revealing view of a potential femoroacetabular impingement deformity.
Multiple studies focusing on prevalence data in femoroacetabular impingement have shown that 24-50% of asymptomatic patients have radiographic signs of femoroacetabular impingement. These data highlight the importance of clinically correlating imaging when assessing a patient who might have femoroacetabular impingement.
In Cam impingement, alpha angle is a commonly used quantitative measure of the deformity. This angle is determined by placing a circle over the femoral head with a line from the center of the circle to the center of the femoral neck and another line from the center of the circle to the first point of the superior head-neck junction (Figures 9 and 10).
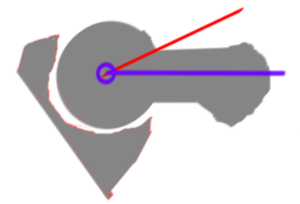
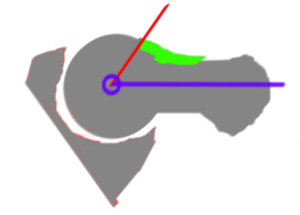
The higher the angle between these two lines, the larger and more severe the Cam lesion. However, there is no precise criterion value for alpha angle that defines pathological abnormality and (interestingly) the original paper in Clinical Orthopaedics and Related Research describing femoroacetabular impingement did not mention the alpha angle.
Alpha angles are most accurate when obtained from special MRI scans which control for hip rotation.
Radiographs in Pincer type impingement reveal acetabular over coverage on the AP pelvis plain film. There may also be retroversion of the femoral neck.
A classic finding of Pincer impingement due to acetabular retroversion is the crossover sign, in which the anterior rim of the acetabulum crosses the line of the posterior aspect of the rim prior to the lateral aspect of acetabulum
Center edge angle is another measurement used to assess for acetabular over coverage leading to Pincer type impingement.
Epidemiology
Labral tears have the highest incidence in patients with acetabular dysplasia.
Cam impingement anatomy is more commonly seen in young males. Pincer lesions are more frequently seen in middle-aged females.
The most common subtype of femoroacetabular impingement is combined, or a component of both Cam and Pincer impingement.
Needless to say, all anatomic measures, including the roundness of the proximal femur and amount of anterior acetabular coverage lie on a continuum, with no perfect criterion separating normal from abnormal. With a sufficiently lax definition, nearly all people have some degree of femoroacetabular impingement anatomy.
Differential Diagnosis
There are numerous pathologies that can lead to pain at the hip or groin. Extra-articular injury of muscles and tendons are the most common source of hip and groin pain in young active adults. Thus, one must consider muscle strains and tendinopathies.
Snapping hip may produce symptoms resembling mechanical hip pain seen in femoroacetabular impingement or labral tear. Bursitis, particularly iliopectineal bursitis, produces groin pain and increased pain with hip flexion.
Neuropathies should also be included in the differential for hip/groin pain. While obturator or ilioinguinal nerve entrapments may cause discomfort in the groin, these conditions often are associated with paresthesias or neurologic symptoms.
Stress fractures of the femoral neck and pubic rami must also be considered in patients presenting with hip/groin pain especially in thin long-distance runners.
Osteitis pubis (inflammation of the pubic symphysis) and groin muscle strains (also known as athletic pubalgia or “sports hernia”) may cause hip pain similar to that of labral tears.
Hip osteoarthritis can cause groin pain, especially in older patients.
Red Flags
A stress fracture of the femoral neck may be the source of the presenting complaints and should not be missed. Pain that is related to activity and not changed by position of the hip joint should increase the suspicion of this diagnosis, especially in patients at risk for stress fractures.
Treatment Options and Outcomes
Nonoperative treatment, centering on rest, anti-inflammatory pain medications and physical therapy, should be the initial treatment for most patients with labral tears. While no universal physical therapy regiment has been defined, plans of rehabilitation focusing on hip strength and mobility in conjunction with posture and core strength have intuitive appeal.
Intra-articular hip injections can be considered but their efficacy has not been proven. A lack of a response to a preoperative injection is predictive of poor short term surgical outcomes.
Operative treatment of labral tears can involve labral resection, re-fixation, or reconstruction of soft tissue. However, studies have shown labral re-fixation results in better outcomes and decreased cartilage degeneration in comparison to resection.
Because of the high prevalence of femoroacetabular impingement morphology in asymptomatic patients, it is speculative at best to suggest that any treatment should be employed in the name of altering the risk of arthritis later in life. It may be more reasonable to address femoroacetabular impingement bony deformities when surgery is undertaken to repair the labrum: osteoplasty of the Cam deformity or resection of the Pincer lesion may be chosen.
Risk Factors and Prevention
Hip dysplasia is the most common cause/risk factor for developing a labral tear.
According to the classic report on femoroacetabular impingement, “patients with otherwise normal or near-normal anatomic structure of the hip [can] experience impingement as a result of subjecting the hip to excessive and supraphysiologic ROM.”
A history of a slipped epiphysis can lead to femoral neck retroversion and place patients at a risk for Cam impingement. Likewise, acetabular protrusion and coxa profunda predispose patients to Pincer impingement.
Key Terms
Femoroacetabular impingement, cam lesion, pincer lesion, hip labrum
Skills
Perform physical examination to suggest or exclude the diagnosis of labral disease.
