3 Spondylolysis and Spondylolisthesis
Spondylolysis and spondylolisthesis are relatively common causes of low back pain, especially in young athletes. Spondylolysis refers to a weakening or other defect in a specific region of the vertebra called the pars interarticularis. These defects may be caused by repetitive stress. Spondylolisthesis refers to anterior slippage (displacement) of the vertebrae. This is often the result of bilateral spondylolysis, a so-called isthmic spondylolisthesis. Thus, spondylolysis and spondylolisthesis are separate yet interrelated conditions.
Besides isthmic spondylolisthesis, there are several other notable subtypes of spondylolisthesis. The two other most common forms are degenerative spondylolisthesis and dysplastic (congenital) spondylolisthesis. Less common forms include traumatic, pathologic, and iatrogenic/post-surgical.
Structure and Function
The human spine has 24 vertebrae stacked one on top of the other: seven cervical, twelve thoracic and five lumbar. The lowest lumbar vertebra, L5, sits atop the sacrum. The vertebral bodies are separated by intervertebral discs, which function both as elastic bearings permitting motion as well as shock absorbers dissipating forces transmitted through the spinal column.
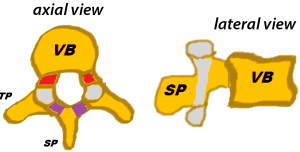
Behind the vertebral body lie the so-called posterior elements of the spine: the pedicles, the lamina and three processes: the transverse, the articular, and the spinous processes (Figure 1). The posterior elements connect to the vertebral body via the pedicles. At the dorsal limit of the pedicle is the pars interarticularis. The pars then extends cephalad to become the superior articular process and caudad to become the inferior articular process. The transverse process projects laterally from the pars in the thoracic and lumbar spine. Coursing dorsally from the pars, the laminae extend dorsally and medially to connect in the midline and complete the ring around the spinal canal. The spinous process is a dorsal extension from the junction of the two laminae at the midline.
Damage to the pars can incite an attempt at healing. The resultant hypertrophic fibrous tissue can cause foraminal stenosis with compression of the exiting nerve root. This most commonly occurs at L5-S1, resulting in an L5 radiculopathy.
On each side, left and right, the inferior articular processes of the vertebra above and the superior articular processes of the vertebra below, come together to form the facet joints. The function of the facet joint is to guide and also limit motion of the spine. Specifically, the facet joints in the lumbar spine permit flexion, extension, and rotation while simultaneously preventing extremes of these motions as well as translation.
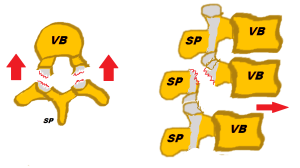
Because the pars bridges the articular processes to the vertebral body, damage to the pars results in functional incompetence of the facet joints. It is this loss of restraint that allows anterior displacement or “slippage” of the superior vertebral body: spondylolisthesis (Figure 2).
In the vast majority of cases, spondylolysis is a developmental defect that may be present in up to 5-7 percent of the population and is typically asymptomatic. In the setting of new onset low back pain, spondylolysis may occur from overuse causing microfracture. In rare circumstances, a fracture in the pars articularis can occur following an acute load or trauma.
While the progression from a pars defect to spondylolisthesis is the mechanism of isthmic type spondylolisthesis, the pathophysiology of degenerative spondylolisthesis is different. In the most fundamental sense, the major difference between isthmic and degenerative forms is the absence of a defect in the pars interarticularis causing the anterior displacement in degenerative spondylolisthesis. Instead, the pathophysiology in degenerative spondylolisthesis centers around degeneration of the facet joint and intervertebral discs, leading to instability and increased motion of the vertebra. Degenerative spondylolisthesis is most commonly seen at L4-L5. Because the pars remains intact, the posterior elements of the sliding vertebra must also slide as a unit. Thus, degenerative spondylolisthesis is more likely to result in stenosis within the canal (especially the subarticular region) affecting the traversing roots. This contrasts with the isolated foraminal stenosis typically encountered with isthmic spondylolisthesis.
With respect to the other, rarer forms of spondylolisthesis, the dysplastic (congenital) type occurs secondary to abnormal spine development in utero, traumatic is the result of severe traumatic injury leading to vertebral displacement, and pathologic refers to the presence of a secondary disease process resulting in instability and displacement of the vertebra, including osteoporosis, malignancy, or infection.
Patient Presentation
The diagnosis of spondylolysis is often an incidental discovery on an x-ray without any clinical signs or symptoms. In fact, the majority of patients with radiographic evidence of spondylolysis are asymptomatic.
In patients with spondylolysis that have symptoms, however, the most common complaint is low back pain of gradual onset that is worsened with activity, especially activities which involve hyperextension of the lumbar spine. The quality of the pain is non-specific and may resemble that of an ordinary lumbar muscle strain.
The presentation of isthmic spondylolisthesis is similar to that of spondylolysis, with non-specific low back pain often being the primary complaint. In spondylolisthesis, however, there is a higher occurrence of radicular symptoms. Impingement of the L5 nerve root in the foramen is most common, resulting in radiculopathy (paresthesias or pain radiating to the legs, or “sciatica”).
In rare circumstances, patients with spondylolisthesis can experience a “listhetic crisis” characterized by severe back pain, neurologic deficits, and hamstring spasm, all which may be exacerbated by extension of the lumbar spine.
On physical examination of patients with spondylolysis and spondylolisthesis, there may be evidence of increased lumbar lordosis (inward curvature of the spine), decreased range of motion of the spine, pain upon lumbar spine extension, or a palpable step off of the spinous process (representing anterior displacement in spondylolisthesis). They may also have sensory or motor findings on neurologic exam depending upon any underlying neural compression.
In degenerative spondylolisthesis, low back pain is the most common symptom as well. These patients, however, may experience neurogenic claudication and leg pain secondary to spinal canal stenosis, which is more common in the degenerative than the isthmic form.
Objective Evidence
The gold standard modality for the diagnosis of spondylolysis and spondylolisthesis are plain radiographs of the lumbar spine. The important views are standing anterior-posterior (AP) and lateral in the standing position. Oblique views may also be obtained, but these are unnecessary in most cases.
In the AP view, sclerosis of the pars interarticularis may be appreciated secondary to stress reaction. From the lateral view, a defect in the pars interarticularis is identifiable in the majority of cases (Figure 3).

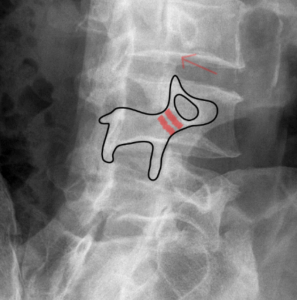
The oblique film is a more specific view in the assessment of spondylolysis and spondylolisthesis. From this angle, the vertebra in the lumbar spine demonstrate the classic “Scottie dog” appearance (Figure 4), consisting of the superior articular process (ears of the dog), transverse process (head), isthmus (neck), lamina and spinous process (body), and inferior articular processes (foreleg and hindleg). In spondylolysis, the defect in the pars interarticularis appears as a neck collar on the Scottie dog.
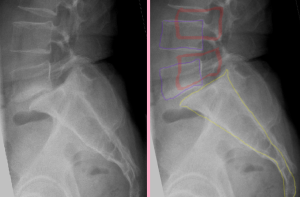
In spondylolisthesis, there is relative anterior displacement of the superior articular process, allowing the entire body to slip forward (Figure 5).
Spondylolisthesis can be graded based on magnitude of vertebral displacement. The superior endplate of the caudal vertebra is divided into quarters. The grade is dependent on location of the poster-inferior corner of the vertebra above. Grade 1 represents a 0-25% displacement, grade 2: 25-50%, grade 3: 50-75%, and grade 4: > 75%. Grades 1 and 2 are considered ‘low grade’ and grades 3 and 4 are considered ‘high grade’. This distinction is important when developing an appropriate treatment strategy.
Advanced imaging may also play a role in the assessment of spondylolysis and spondylolisthesis in select circumstances. CT scan is the best modality for revealing the specific anatomy of the underlying lesion in spondylolysis, and thus can be helpful for delineating subtle defects. In patients with neurologic complaints or deficits on examination, MRI is warranted to further assess for neural element impingement. Bone scan (SPECT) is also highly sensitive for spondylolysis, and may be utilized in patients with a high suspicion for a pars defect with normal or inconclusive radiographs in whom cross-sectional imaging is undesirable.
Epidemiology
While the precise etiology of spondylolysis remains unknown, the pars defects typically occur in childhood or adolescence as an acquired phenomenon, as true congenital spondylolysis is exceedingly rare. This anatomic variant is present in 5 to 7 percent of the entire population, but can occur in as many as 45 percent of pediatric athletes involved in high risk sports. (High risk activities include gymnastics, Olympic weightlifting, football, dancing, figure skating, and wrestling.) This is currently the most common identifiable source of low back pain in adolescents.
Progression of spondylolysis to spondylolisthesis is uncommon, occurring in less than 15 percent of patients. Certain anatomic risk factors can help predict which patients are at increased risk of progressive listhesis.
L5-S1 is the most commonly affected spinal segment in isthmic spondylolisthesis (90%), followed by L4-L5 (10%).
Degenerative spondylolisthesis occurs in older adults. In the majority of cases, this occurs after the age of 40, though risk increases upon increasing age.
Isthmic spondylolisthesis is slightly more common in males, while degenerative spondylolisthesis is significantly more common in females (about eight times more prevalent) and occurs in approximately 10% of all women.
Differential Diagnosis
In the patient with unknown spondylolysis or spondylolisthesis presenting with low back pain, the differential diagnosis is broad. In the pediatric patient, this includes lumbar disc related pathology, lumbar muscle strain, Scheuermann’s kyphosis, scoliosis, sacroiliac joint dysfunction, tumors (including especially osteoid osteoma), or infection (vertebral osteomyelitis or discitis). In the older patient, the differential diagnosis is similar but also includes degenerative disc disease or spinal stenosis without spondylolisthesis.
In a patient with confirmed spondylolisthesis, the differential diagnosis revolves around the specific etiology, and includes the six different types: dysplastic, isthmic, degenerative, traumatic, pathologic, and iatrogenic.
Red Flags
Pain that fails to relieve predictably with rest (“night pain”) and associated constitutional symptoms (fever, chills, unintended weight loss) are always red flags for further investigation to avoid delays in making important diagnoses, such as malignancy or infection.
Signs or symptoms of cauda equina syndrome, which is a surgical emergency, include bowel or bladder incontinence, saddle anesthesia, and progressive lower extremity weakness. (Note that cauda equina compression from a high-grade listhesis requires translation of the posterior elements and laminae along with the body. Accordingly, compressions is highly unlikely in the setting of true isthmic spondylolisthesis.
Treatment Options and Outcomes
The primary goal of treatment of spondylolysis is resolution of symptoms and return to activity. Radiographic healing of the pars defect may or may not correlate with the resolution of symptoms and is of secondary importance in the setting of isolated spondylolysis or low-grade spondylolisthesis.
There are three general categories of management strategy for patients with spondylolysis and spondylolisthesis: symptomatic treatment with analgesics and observation without activity modification/limitation (benign neglect); activity modification/limitation with or without bracing; and surgical intervention.
Benign neglect is most appropriate for asymptomatic or minimally symptomatic patients with isolated spondylolysis or low-grade spondylolistheses.
Activity modification is generally indicated for patients with spondylolysis or low-grade spondylolisthesis who are symptomatic. This strategy encompasses use of NSAIDs for pain control and physical therapy with a focus on stretching, lumbar spine flexion, core strengthening/stability as first-line.
For radicular pain that fails to improve with time and NSAID use, steroid injections may be a useful alternative.
Lumbar spine bracing may also be beneficial, particularly in the case of a failed trial of physical therapy or in an acute pars stress reaction spondylolysis, for which bracing is superior to activity restriction alone.
Surgical management is the final line of therapy for spondylolysis and spondylolisthesis. Surgery is rarely required for isolated spondylolysis without spondylolisthesis. Broadly, the major indications for surgery include refractory radicular symptoms, a progressive neurologic deficit, high grade progressive spondylolisthesis, and intractable pain or disability despite exhaustive non-operative management.
The goal of surgery for spondylolisthesis is to stabilize the unstable segment. This can prevent slip progression and reduce back or leg pain. Direct repair of a pars fracture may be considered in the absence of listhesis and at levels L4 and above in an effort to preserve lumbar motion. In degenerative spondylolisthesis, surgical options also typically include decompression (to address neural impingement) with or without concurrent fusion.
In general, the prognosis of spondylolysis and spondylolisthesis is very favorable. For symptomatic patients who undergo non-operative or operative treatment, the vast majority experience total relief of their pain and regain full functionality.
For patients with symptomatic spondylolysis, the majority will improve with observation and non-operative management. Only 15% of patients with spondylolysis will go on to develop spondylolisthesis.
For spondylolisthesis, the outcome is dependent upon grade/severity and specific subtype. Since most cases of spondylolisthesis are low grade, the overall prognosis is good. In these mild cases, non-operative management is successful in about 80% of patients. With regard to risk for displacement progression, dysplastic portends the highest rate (over 30%), while the most common type (isthmic) progresses in less than 5% of cases.
Severe spondylolisthesis portends a slightly worse prognosis, but the prognosis is still favorable overall. There is a higher risk of neurologic damage secondary to nerve compression, in addition to the risks associated with surgery (below). There is also a higher likelihood of persistent low back pain and disability, though surgery is successful in 85-90% of cases.
Specific complications of surgery include mainly pseudoarthrosis, infection, dural tear, neurologic deficits, and instrumentation (ie, the surgical hardware) failure. The risk of complications is generally higher for patients with degenerative spondylolisthesis given their increased age and medical comorbidities.
Note that excessive avoidance of activity may also impose costs on patients including deconditioning, weight gain, osteoporosis, and psychologic distress. It may be possible, thus, to be excessively conservative in recommending treatment.
Risk Factors and Prevention
The primary risk factor for spondylolysis and spondylolisthesis is frequent hyperextension of the lumbar spine. Participation in sports such as gymnastics and football (and others in which the spine is extended) is associated with a higher prevalence of defects in the pars interarticularis.
The best approach for preventing spondylolysis is to avoid repetitive hyperextension of the lumbar spine. In addition, maintaining core muscle strength, flexibility and good bone health are important.
Key Terms
Spondylolysis, spondylolisthesis, facet joint, pars articularis, ‘Scottie dog’, spinal fusion
Skills
Understand the similarities and differences in the pathophysiology underlying spondylolysis and spondylolisthesis. Recognize the different subtypes and severity grading system for spondylolisthesis. Understand the non-operative and operative treatment modalities and their efficacy in the treatment of spondylolysis and spondylolisthesis.
