19 Patellofemoral Disorders
Anterior knee pain may be found with patellar instability (subluxation or complete dislocation of the patella out of the trochlear groove) or patellofemoral arthrosis. It may also have no objectively defined cause, in which case the label “patellofemoral pain syndrome” is applied. Many patients with patellofemoral pain syndrome improve with no treatment. Patellar instability may be treated with muscle strengthening therapy or braces; at times, however, surgery is needed.
Structure and Function
The patellofemoral joint is formed by the patella and the anterior surface of the distal femur, an area called the trochlear groove.
The patella is a sesamoid bone that is embedded within the quadriceps tendon and serves to increase the mechanical advantage of the quadriceps muscle. The undersurface of the patella is composed of two main facets, lateral and medial. The lateral facet is longer and less steep, matching the geometry of the lateral aspect of the trochlea.
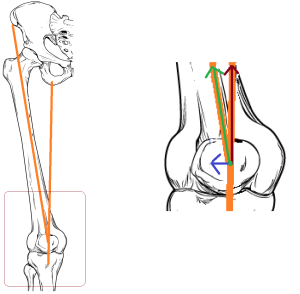
Stability of the patella in the patellofemoral joint relies on normal trochlear morphology of the femur. The trochlear groove must be sufficiently deep to hold the patella, especially in flexion. Stability also depends on the alignment of the tibia relative to the femur. A so-called valgus or “knock-knee” alignment of the knee joint increases the lateral vector of the quadriceps. If the lateral vector is too great, the quadriceps can pull the patella out of the trochlear groove, especially as the knee nears terminal extension. This can be assessed by two measurements: the angle between the quadriceps and the infrapatellar ligament, so-called Q angle and the tibial tubercle to trochlear groove (TT-TG) distance (Figure 2).
Additional static stability is provided by the lateral retinaculum, medial retinaculum, medial patellofemoral ligament, and medial patella-tibial ligament.
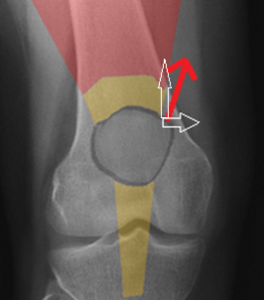
The vastus medialis obliquus provides dynamic stability, actively pulling the patella medially, to keep it located within the joint (Figure 4).
During initial knee flexion (<30 degrees), the major restraints to lateral translation and dislocation are the soft tissue structures; beyond 30 degrees, the bony structures are the primary determinants of stability.
The medial patellofemoral ligament is the primary soft tissue restraint against lateral translation of the patella. This ligament is torn when there is excessive lateral translation of the patella.
In cases of so-called patella alta, a longer than normal patellar tendon allows the patella to rest more proximally. As a result, the patella does not enter the trochlear groove until higher-than-normal levels of knee flexion have occurred. In patients with recurrent instability, trochlear dysplasia has been noted to be present in up to 96% of patients.
Patient Presentation
A thorough patient history and physical examination are critical components in diagnosing patellofemoral pain syndrome and patellar instability. Patients will report pain and possibly swelling in their knee with increasing intensity such as climbing or descending stairs, squatting, running, jumping, or “cutting” during sports activities.
In some cases of patellofemoral pain syndrome, patients will commonly report feeling pain “behind,” “underneath,” or “around” the patella. Many patients will not experience swelling with patellofemoral pain syndrome; however, patients will note stiffness, particularly when the knee is flexed, as well as potentially “popping” or “catching” sensations.
Patients may also note overall weakness in their leg as well as a feeling that their knee might “give way” again in cases of patellar instability. Discoloration medially and pain along the medial aspect of the knee are commonly seen. The number of prior identifiable dislocations and subluxation episodes for the patient as well as any history of ligamentous laxity or dislocation of family members must be noted.
Physical examination should note alignment and range of motion; the presence or absence of tenderness should be noted as well.
Examination maneuvers are shown in the figures 5-8.

(Note that these maneuvers are performed in sequence, not simultaneously. For the two tests, the position of the patient and the examiner are the same, with the only difference being the motion of the examiner’s thumb, hence a single photo is shown. These test do address a unified issue: namely, can the patella be moved passively a “normal” amount?)


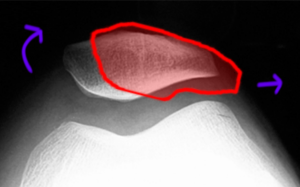
Figure 8: Patellar tracking (J-sign): The examiners scrutinizes the position of the patella when the knee moves from full flexion (top panel) to mid-flexion (middle panel) and then extension (bottom panel). In full flexion, the patella, outlined in red, will be located in the trochlea groove even if the soft tissues are lax; but in the setting of laxity, the patella will move to a lateral position in extension. Thus, if the soft tissues are lax, the patella will follow a “J” or “L” course when the knee moves from flexion to extension, or vice versa (left vs right). In the figure, the model is normal, and no “J” sign is demonstrated: the patella remains central. |
Most patella dislocations occur laterally; therefore, the lateral patellar apprehension test represents the best test for determining patellar instability.
The quadriceps and patellar tendons should be palpated to detect tendinosis.
Additionally, a Lachman’s test, pivot shift, anterior and posterior drawer test, dial test, and varus/valgus stress test should be performed to rule out other injuries.
Objective Evidence
Patellofemoral pain syndrome is primarily a clinical diagnosis and can be made without radiographic imaging. Nevertheless, x-rays will commonly be ordered to rule out structural abnormalities.
In cases of suspected patella instability, anteroposterior and posteroanterior 45° weight bearing views should be obtained to examine any abnormal anatomy, particularly current presence of dislocation. Lateral radiographs should be ordered to examine patella height, trochlear dysplasia and patellar tilt.
The sunrise view (Figure 9) can evaluate for lateral subluxation and patellar tilt.
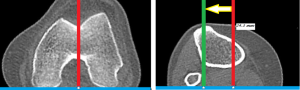
CT scans provide valuable axial information allowing evaluation of the anterior tubercle to trochlear groove distance. The mean tibial tubercle to trochlear groove distance has been noted to be 9 mm while a tibial tubercle to trochlear groove distance of 20 mm or more has a 90% association with patellar instability. CT is more reliable than MRI for this assessment.
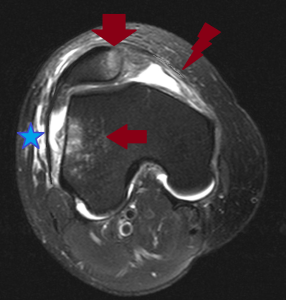
MRI is valuable in assessing for cartilage/osteochondral injury as well as soft tissue structures of the knee. MRI will help evaluate any articular cartilage damage on the medial facet of the patella and bone bruising of the lateral femoral condyle.
Epidemiology
Anterior knee pain is the most common knee diagnosis in sports medicine centers and among runners. Up to 11% of musculoskeletal complaints in the outpatient setting are caused by anterior knee pain, most commonly patellofemoral pain syndrome, and the incidence of patellofemoral pain syndrome in runners is between 16% and 25%.
The majority of patellar instability occurs in young, active individuals with an incidence of 1 per 1000 people. Overall, patellar dislocations represent approximately 3% of all knee injuries. Females are more likely to have patellar dislocations than men and the most commonly affected age group is individual’s ages 10 to 16 years old. Patellar instability is commonly traumatic in nature due to either contact or non-contact mechanisms; however, patients with patellar malalignment may experience frequent low-energy patellar dislocations.
Differential Diagnosis
Anterior knee pain may be due to instability (with or without an overt history of dislocation); it may be due to patellofemoral arthrosis (with or without radiographic confirmation); it may be due to tendinosis on either side of the patella; or it may have no known causes.
At times, patellar dislocations reduce spontaneously, such that the patient may not be aware that the patella dislocated other than feeling a shift in their knee.
Patients may report buckling due to patellar inhibition, but of course true ligamentous laxity must be excluded before that diagnosis is credited.
Red Flags
Gross laxity of the patellofemoral stabilizers may suggest a connective tissue disorder, such as Ehlers-Danlos syndrome.
Incomplete passive motion after a patellofemoral dislocation suggests a loose body within the knee.
Treatment Options and Outcomes
For patients diagnosed with patellofemoral pain syndrome, a comprehensive rehabilitation program is the first line of treatment. Rehabilitation programs should include modification or cessation of activities as well as physical therapy.
A knee sleeve, splint, or taping may be used as well. This may help hold the patella within the trochlea. Alternatively, these may help simply by serving to remind the patient to avoid full flexion.
Recovery from patellofemoral pain syndrome can take longer than most patients anticipate.
Patients with pain but without a correctable anatomic lesion are rarely helped (and may be hurt) by surgery.
Patients sustaining their first dislocation can be treated with a brace. However, even in first time dislocations (especially if there is a large hematoma that raises concern for osteochondral injury) – an MRI is useful. This test can detect loose bodies and assess for any damage to the ligaments and cartilage.
After a first-time dislocation, physical therapy (PT) is started 1-2 weeks after the dislocation, to help achieve normal range of motion and strength and is continued for 2-3 months. In some cases, 4-5 months of PT is necessary in order for athletes to return to their pre-injury level of activity.
In cases of recurrent instability, operative treatment is frequently recommended. Operative treatment is based upon the patient’s anatomy and the spectrum of injury. It may consist of either an isolated soft tissue procedure or a bony realignment procedure or both.
The most common procedure is reconstruction of the medial patellofemoral ligament with an autograft (hamstring tendon) or allograft. Although less common, repair of the medial patellofemoral ligament is possible in some patients who seek treatment promptly and have a bony avulsion of the ligament from the medial aspect of the patella.
In cases of recurrent instability where the distance between the tibial tubercle and the trochlear groove is greater than 20 mm, an osteotomy of the tibial tubercle is needed. In this operation, the tubercle is moved medially, to realign the patellar tendon and in turn make the patella track more medially.
For patients with an open growth plate, surgeons will commonly perform an isolated soft tissue procedure and then perform the realignment surgery after closure of the growth plates to prevent further cartilage damage underneath the kneecap as well as to prevent arthritis from developing.
In cases of extreme dysplasia, operations to deepen the base of the trochlea or elevate the lateral facet (so-called trochleoplasty procedures) may be performed. This approach has not gained widespread acceptance among orthopaedic surgeons.
For either procedure, rehabilitation typically lasts 4-6 months post-surgery and final recovery and return to sports is not usually achieved until after 6 months from reconstruction (when full range of motion, stability, and strength have been restored).
Following completion of a thorough rehabilitation program, patellofemoral pain syndrome commonly resolves–but to prevent recurrence, appropriate conditioning of the muscles around the knee, particularly the quadriceps and the hamstrings is essential.
After an initial dislocation, the ligaments are stretched from the injury; therefore, patients are at an increased risk for either a recurrent subluxation or dislocation. The incidence of recurrent instability following conservative treatment has been noted to be between 15% and 44%. After a second dislocation, the risk of recurrence increases to over 50% and in younger patients (less than 25 years of age, particularly those with open growth plates) the risk of recurrence after a second dislocation has been noted to be as high as 70%.
Following operative treatment, the success rate for stabilization has been noted to be as high as 85% – 90% for both soft tissue and bony procedures.
Risk Factors and Prevention
Risk factors for patellofemoral pain syndrome include females and young adults as the condition is commonly referred to as “runner’s knee”, due to the high occurrence in athletes. Additionally, malalignment of the kneecap and overuse from vigorous athletics or training are also significant risk factors.
For patellar instability, risk factors include young age (under the age of 25 with a peak incidence between ages 10-16 years old) and open growth plates (this is particularly a risk factor for patients after primary dislocation). A prior history or patellar dislocation or subluxation represents a significant risk factor as up to 44% of patients treated conservatively may experience a second instability episode.
Key Terms
Patellar dislocation, patellar subluxation, medial patellofemoral ligament injury, Q-angle, tibial tubercle to trochlear groove distance, trochlear dysplasia, patella alta
Skills
Perform Patellar, tilt, apprehension and inhibition tests. Assess Q angle on imaging.
