Chapter 10: Relationships, Sexuality, & Contraception
How does social health impact overall health?
What does it mean to love?
How can I know whether my relationship is healthy or unhealthy?
What can I do to be en effective communicator?
What type of birth control is best for me?
Chapter 10 Learning Outcomes
By the end of this chapter you will be able to:
- Compare signs of health and unhealthy relationships
- Define the many types of loving relationships.
- Employ effective communication techniques.
- Describe the difference between sex, gender, and sexuality
- Choose the best type of contraceptive method based on effectiveness against unintended pregnancy and STD transmission.
Relationships
Social wellness is just one of the dimensions of wellness that impact our overall health and well-being. Maintaining healthy relationships, enjoying being with others, developing friendships and intimate relations, caring about others, letting others care about you, and contributing to your community are all important aspects of developing your social wellness. A meta-analysis of 148 studies indicated that people with adequate social relationships had a reduction in risk of mortality comparable to quitting smoking[1] and social relationships have also been shown to prevent and even cure some diseases[2], thus it is well documented that strong social relationships extend life and improve health.
Types of Relationships and Love
It is challenging to define what love is and the varying types of love and relationships we have throughout our life. A Psychologist named Robert Sternberg has spent is career researching love and developing theories that help increase our understanding of love and relationships.
Triangular Theory of Love
In the 1980’s, Sternberg developed the Triangular Theory of Love[3] which describes different types of love and relationships based on a combination of three components (ingredients): passion, intimacy, and commitment. Years later Sternberg developed the Theory of Love as a Story, which focuses on how a persons beliefs and conceptions about relationships impact the type and success of their relationships. Most recently, Sternberg has blended the two theories into one theory now known as Sternberg’s Love-Match Theory.
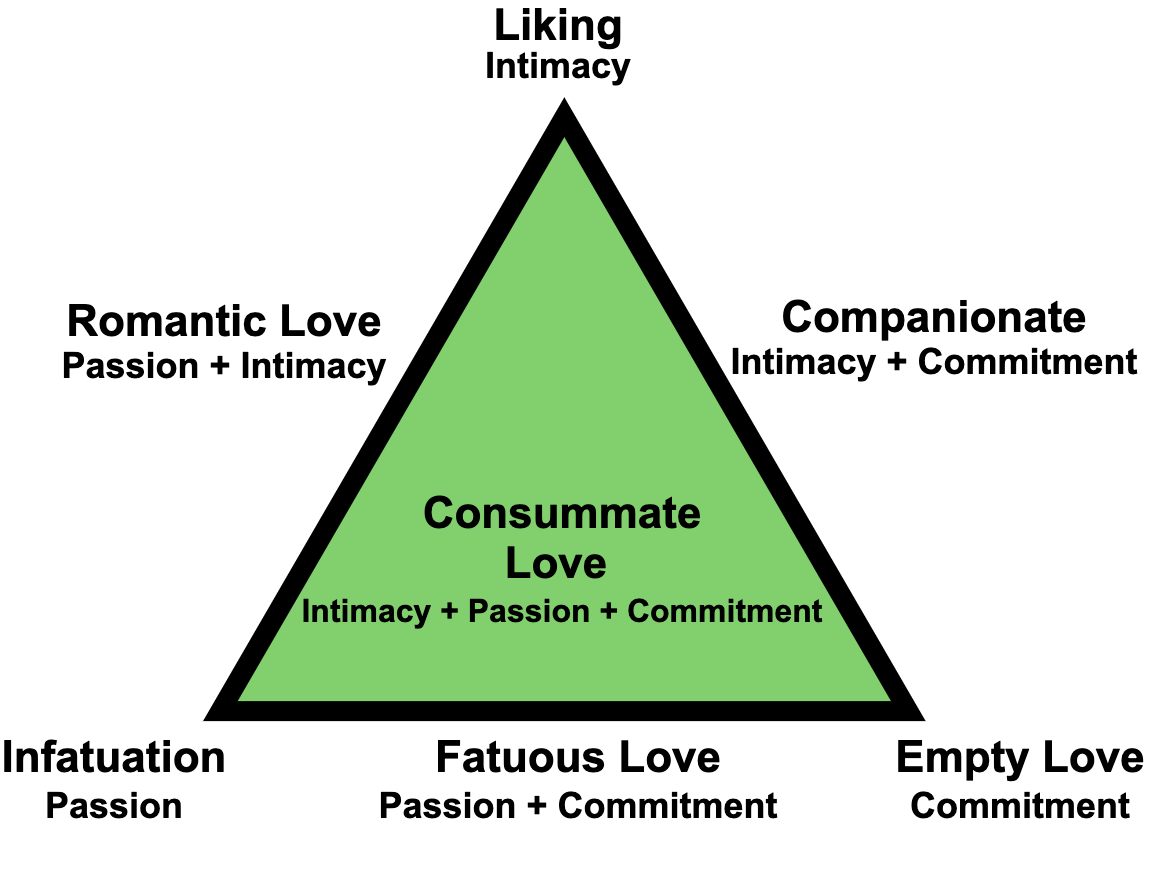
Sternberg uses intimacy, passion, and commitment to describe different types of love, with each type of love including varying degrees of intimacy, passion, and commitment. The goal for a long term happy relationship is to have a high level of all three components.
- Intimacy refers to feelings of closeness, connectedness, and bondedness. Feeling warmth, feeling comfortable to be open an honest, feeling that you are valued and safe, and feeling that you can count on the person.
- Passion typically refers to the drives that lead to romance, physical attraction, or sexual fulfillment. However, passion can also refer to intense feelings of care, such as not being able to live without the person, which could be a passionate need to ensure someone is safe and healthy, like a child or family member.
- Commitment is not a feeling, but rather a decision you choose to make throughout your relationship. It is the decision to love a certain person, and in the long-term, to one’s commitment to maintain that love.
| Type of Love | Intimacy | Passion | Commitment |
| Non-Love | No | No | No |
| Friendship | Yes | No | No |
| Infatuation | No | Yes | No |
| Empty Love | No | No | Yes |
| Romantic Love | Yes | Yes | No |
| Companionate Love | Yes | No | Yes |
| Fatuous Love | No | Yes | Yes |
| Consummate Love | Yes | Yes | Yes |
Reflection: Types of Love in Your Life
Review the types of love in Table 10.1. Identify people in your life or in your past who you would associate with each type of love.
Think about a relationship you’ve been in…
- How has the type of love changed over time?
- How might you use the varying levels of passion, intimacy, and commitment to identify areas of a relationship that may need work?
Theory of Love as a Story
Although the Triangular Theory of Love provides a helpful structure for understanding varying types of love, it does not account for a persons belief in what love is or should be. Sternberg’s Theory of Love as a Story focuses on recognizing and understanding a persons “love story” and how that story impacts their relationships. By understanding our story and the story of potential partners we can better understand the expectations for the relationship.
A persons love story is unconsciously developed throughout their life by the relationships they see in real life as well as through media. Your love story helps to explain what you are seeking in loving relationships and how that relationship fulfills your needs and wants. Although there are infinite story possibilities, based on years of research Sternberg identified 26 types of love stories including the garden story, business story, sewing story, horror story, sacrifice story, art story, and game story [4][5].
Each type of story describes the relationship dynamics that are commonly at play. For example, those with a Business Story of relationships view the relationship as a business proposition or transaction and are looking for a business partner who will keep life organizes and focused on important things like the economy, money, and social status. However, persons with a Garden Story of relationships view the relationship as something that will is successful as long as you take care of it and nurture it to grow strong, so for these persons it is important to take care of each other and take care of their relationship.
Research indicates that similar or complementary love stories lead to more successful relationships; Similar love stories mean each person is bringing similar expectations to the relationship. With this understanding, it may be helpful to more fully understand your own love story and also to recognize and understand the love story of your partner. Once we recognize and understand our own love story, we can begin to ask ourselves if we like the story, if the story has been working for us, or if we would like to change our story.
Challenge: Love Stories and Movies
Sternberg describes 26 types of love stories and explains that we see these love stories in various media throughout our lives.
- Review the 26 types of love stories and try to associate a type of love story with a relationship as depicted in a movie you’ve watched or a book you’ve read.
- In what ways were you able to identify the type of love story each person brought to the relationship?
- Did both people in the relationship bring a similar love story to the relationship?
- Were you able to identify relationships where two people brought different love stories, or expectations, to the relationship? Did it cause a conflict?
Healthy vs. Unhealthy Relationships
We know relationships are important to our health and well-being, however not all relationships are good for us. It is important to understand the signs and characteristics of healthy and unhealthy relationships.
In a healthy relationships, the couples believe in non-violent conflict resolution, where they can talking honestly, can agree to disagree, and make decisions and compromises together. They communicate effectively ensuring they are listening to each other without judgement and communicate respectfully showing each person is valued and loved. They recognize that each person is a unique individual and respect their right to autonomy to able to enjoy time apart with friends and activities they enjoy. Their relationship is based on trust which allows them to feel comfortable being themselves and feel unconditionally supported. Lastly, they have fun together and have more good times than bad.
Unhealthy relationships might include a focus on only one person while disregarding the other. One or both of the people in the relationship might drop friends and family or activities they enjoy. They might feel pressured or controlled in the relationship or often feeling sad, scared, or lonely when together. When a relationship has more bad times than good times, this can be a sign that the relationship is unhealthy.
| Healthy Relationships | Unhealthy Relationships |
|
|
Communication
Being able to effectively communicate is an important skill for successful relationships.
Three keys to Effective Communication are:
- Be an active listener
- Actively listening means listening without judging and with an openness to want to understand what you are hearing.
- Communicate clearly
- When developing either written or verbal communication it is important to take into consideration your audience, their cultures, and their experiences. Communication takes many skills, it is not just about listening and speaking, but also takes into consideration your thoughts and feelings throughout the exchange and how the setting or type of communication impacts the message. When communicating verbally or through written text it is important to ensure your communication is clear and not too complex or lengthy.
- Understand body language
- Non-verbal clues play a large role in the communication process. Non-verbal feedback may be positive such as nodding the head, maintaining eye contact, and leaning in. Non-verbal feedback can also seem to show you are uninterested, such as looking away, turning the body away, or rolling eyes.
“I” Statements vs. “You” Statements
“I” statements can help you focus on and be clear about your own thoughts and feelings, and what it is that you want or need. They may also involve an acknowledgement of the thoughts/feelings/goals of the other person.
The real focus in “I” statements is on the “I feel,” “I want,” or “I think” part of the statement. Identifying your thoughts, feelings, needs, and wants related to a situation will help you to avoid blaming someone else or getting caught up in the emotion of the moment.
“You” statements, on the other hand, tend to place blame or criticize the other person. This typically puts the other person on the defensive, and does not encourage open communication.
For example, saying “I feel worried when you are running late to meet me for dinner and don’t call to let me know” (I statement) vs. “You are always running late, and never bother to let me know” (You statement) will likely result in two very different reactions and conversations! The first statement simply expresses how the person is feeling, whereas the second statement sets a critical and accusatory tone.
Be Assertive
Assertiveness is an honest and appropriate expression of your feelings, thoughts, wants and needs. Acting in an assertive way helps you to stand up for your rights in a respectful manner. It is a way to communicate what you believe, what you want and need, and what is important to you. Assertiveness can sometimes be compared to, or confused with, being aggressive, however aggressive behavior often means standing up for yourself in ways that violate the rights of others and can be demanding, hostile, and blaming.
People often associate the concept of assertiveness with standing up for your rights when you feel that someone has taken advantage of you in a negative way. However, it is also important to recognize that being more assertive can help you to communicate in a positive way in your relationships, which helps to promote mutual respect. Non-Assertive behavior is often submissive, inhibited, passive, and self-denying.
Assertiveness can help you:
- speak up when you have a question or concern,
- say “no” when you don’t want to do something, and
- express thoughts or feelings
Communicating assertively does not guarantee that you will get what you want or need. However, you will have the satisfaction of expressing yourself in a positive, self-advocating way. You will probably feel better about yourself and your communication with others. And, you will increase the probability of getting what you need or want, while also respecting the wants or needs of others.
What keeps people from speaking up in an assertive way?
- Not being clear about what they want and need
- Fear of displeasing others and of not being liked
- Not believing they have the right to be assertive
- Lacking the skills to effectively express themselves
To become more skilled in communicating assertively it is important to practice. You won’t learn how to become a more assertive person just by reading one book or attending one workshop. You can practice with your friends and family. Let them know what you are doing first! Ask for help/feedback on how you’re doing.
- Start Gradually
- In the beginning, don’t try changing your behavior in the most complex or difficult situations. Practice first in the least risky ones.
- Some examples of starting gradually include:
- Returning a purchased item (that you are not satisfied with) to a store for a refund
- Asking your partner/roommate/kids to help empty the dishwasher or take out the garbage
- Suggesting a movie that you would like to watch for an upcoming movie night
- If you start small to enhance your chances of success, you will experience how it feels to express yourself assertively and it will be easier to move onto more challenging situations.
- Keep in mind that no one can read your mind– focus on expressing and communicating what is important to you.
Sex, Gender, & Sexuality
When filling out official documents, you are often asked to provide your name, birthdate, and sex or gender. But have you ever been asked to provide your sex and your gender? It may not have occurred to you that sex and gender are not the same. However, sociologists and most other social scientists view sex and gender as conceptually distinct. Sex denotes biological characteristics and exists along a spectrum from male to female. Gender, on the other hand, denotes social and cultural characteristics that are assigned to different sexes. Sex and gender are not always synchronous, meaning they do not always line up in an easy-to-categorize way.
Sex
“Sex” refers to physiological differences found among male, female, and various intersex bodies. Sex includes both primary sex characteristics (those related to the reproductive system) and secondary sex characteristics (those that are not directly related to the reproductive system, such as breasts and facial hair). In humans, the biological sex of a child is determined at birth based on several factors, including chromosomes, gonads, hormones, internal reproductive anatomy, and genitalia. Biological sex has traditionally been conceptualized as binary in Western medicine, typically divided into male and female. However, anywhere from 1.0 to 1.7% of children are born intersex, having a variation in sex characteristics (including chromosomes, gonads, or genitals) that do not allow them to be distinctly identified as male or female. Due to the existence of multiple forms of intersex conditions (which are more prevalent than researchers once thought), many view sex as existing along a spectrum, rather than simply two mutually exclusive categories.
Gender
A person’s sex, as determined by his or her biology, does not always correspond with their gender; therefore, the terms “sex” and “gender” are not interchangeable. “Gender” is a term that refers to social or cultural distinctions associated with being male, female, or intersex. Typically, babies born with male sex characteristics (sex) are assigned as boys (gender); babies born with female sex characteristics (sex) are assigned as girls (gender). Because our society operates in a binary system when it comes to gender (in other words, seeing gender as only having two options), many children who are born intersex are forcibly assigned as either a boy or a girl and even surgically “corrected” to fit a particular gender. Scholars generally regard gender as a social construct—meaning that it does not exist naturally, but is instead a concept that is created by cultural and societal norms.
Gender Identity: Cisgender versus Transgender
Gender identity is a person’s sense of self as a member of a particular gender. Individuals who identify with a role that corresponds to the sex assigned to them at birth (for example, they were born with male sex characteristics, were assigned as a boy, and identify today as a boy or man) are cisgender. Those who identify with a role that is different from their biological sex (for example, they were born with male sex characteristics, were assigned as a boy, but identify today as a girl, woman, or some other gender altogether) are often referred to as transgender. The term “transgender” encompasses a wide range of possible identities, including agender, genderfluid, genderqueer, two-spirit (for many indigenous people), androgynous, and many others. The prefix “trans-” comes from Latin, meaning “across from” or “on the other side of”. In contrast, the prefix “cis-” means “on this side of”.
Cultural Variations of Gender
Since the term “sex” refers to biological or physical distinctions, characteristics of sex will not vary significantly between different human societies. For example, persons of the female sex, in general, regardless of culture, will eventually menstruate and develop breasts that can lactate. Characteristics of gender, on the other hand, may vary greatly between different societies. For example, in American culture, it is considered feminine (or a trait of the female gender) to wear a dress or skirt. However, in many Middle Eastern, Asian, and African cultures, dresses or skirts (often referred to as sarongs, robes, or gowns) can be considered masculine. Similarly, the kilt worn by a Scottish male does not make him appear feminine in his culture.
Sexuality
Human sexuality refers to a person’s sexual interest in and attraction to others, as well as their capacity to have erotic experiences and responses. A person’s sexual orientation is their emotional and sexual attraction to particular sexes or genders, which often shapes their sexuality. Sexuality may be experienced and expressed in a variety of ways, including thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships. These may manifest themselves in biological, physical, emotional, social, or spiritual aspects. The biological and physical aspects of sexuality largely concern the human reproductive functions, including the human sexual-response cycle and the basic biological drive that exists in all species. Emotional aspects of sexuality include bonds between individuals that are expressed through profound feelings or physical manifestations of love, trust, and care. Social aspects deal with the effects of human society on one’s sexuality, while spirituality concerns an individual’s spiritual connection with others through sexuality.
LGBTQ+ Health
People who are lesbian, gay, bisexual, transgender, queer, and/or questioning (LGBTQ+) are members of every community. They are diverse, come from all walks of life, and include people of all races and ethnicities, all ages, all socioeconomic statuses, and from all parts of the United States and world. The perspectives and needs of LGBTQ+ people should be routinely considered in public health efforts to improve the overall health of every person and eliminate health disparities.
In addition to considering the needs of LGBTQ+ people in programs designed to improve the health of entire communities, there is also a need for culturally competent medical care and prevention services that are specific to this population. Social inequality is often associated with poorer health status, and sexual orientation has been associated with multiple health threats. Members of the LGBTQ+ community are at increased risk for a number of health threats when compared to their heterosexual peers. Differences in sexual behavior account for some of these disparities, but others are associated with social and structural inequities, such as the stigma and discrimination that LGBTQ+ populations still experience.
LGBTQ+ sexual health and well-being is affected by numerous social and cultural challenges across the life course, contributing to negative health outcomes and posing barriers to attain such protective health indicators as marriage and family formation, community support, and inclusion in faith communities. The incidence of hate crimes and discrimination promulgated through the denial of equal rights contribute to the perpetuation of homophobia as a structural norm.
As a result of cultural and societal discrimination, many LGBTQ+ people suffer an added burden of stress and experience health disparities, such as:
- Potential difficulties in getting or keeping health insurance, and possible employment instability.
- Limited access to high quality health care that is responsive to LGBTQ+ health issues.
- Mental health problems and unhealthy coping skills, such as substance abuse, risky sexual behaviors, and suicide attempts.
- Challenges or difficulties with being open about one’s sexual orientation, which can increase stress, limit social support, and negatively affect overall health.
- The effects of homophobia, stigma and discrimination can be especially hard on adolescents and young adults. In addition to an increased risk of being bullied at school, they are also at risk of being rejected by their families and, as a result, are at increased risk of homelessness.
Whether you are gay or straight, you can help reduce homophobia, stigma, and discrimination in your community and decrease the associated negative health effects. Even small things can make a difference, such as accepting and supporting a family member, friend, or co-worker.
Pregnancy
Pregnancy is the term used to describe the period in which a fetus develops inside a womb or uterus. Pregnancy usually lasts about 40 weeks, or just over 9 months, as measured from the last menstrual period. Health care providers refer to three segments of pregnancy, called trimesters.
Pregnancy begins when a males sperm fertilizes a females egg. When fertilization occurs it is called conception. On average, females release one egg each month, which is called ovulation. Thus, for pregnancy to occur, sperm only has a few days each month where it can meet the egg and attempt to fertilize it. It is important to understand a females menstrual cycle to understand the days where pregnancy is most likely to occur.
It is very important to note that many women have irregular cycle lengths, might ovulate more then once in a month, and might ovulate more than one egg at a time, thus the fertility cycle is not an exact science.
The following description of the fertility cycle is for an average cycle of 28 days.
- Day 1: The first day of menstruation, or period. Periods typically last between 2-7 days.
- Days 1-7: Menstruation
- Sperm can remain alive and viable in the females body up to 5 days after sexual intercourse. So, it’s possible to have intercourse up to 5 days before ovulation and get pregnant as a result.
- Days 12-16: The egg is typically released, called Ovulation, around day 14 of the cycle, however it is best to estimate the release between days 12-16.
- Days 12-17: Once an egg is released from the ovaries, its life span is very short. Conception can only occur if the egg is fertilized 12 to 24 hours after the time of actual ovulation.
These biologic realities mean the actual period of viable fertility can last anywhere from 5 to 8 days. In general, you’re most fertile during the following times:
- the 5 days before ovulation
- the day of ovulation
- within 12 to 24 hours after ovulation
Contraception & Abortion
As you have learned, passion is one of the three components of love, as defined by Sternberg, and relates to physical attraction and sexual desire. When entering into a sexual relationship, it is important to understand the various ways you can protect yourself from unwanted pregnancy and sexually transmitted diseases (STD’s); although all contraceptive methods are intended to reduce unwanted pregnancy, not all of them also protect against STD’s. There are many forms of contraception to choose from whether it is meant to be permanent or temporary (reversible) and whether it prevents pregnancy by either adjusting hormones, placing a barrier between the sperm and egg, or abstaining during ovulation. How effective each method is at preventing pregnancy is impacted by how the couple uses the method. If a person uses the method perfectly, called Perfect Use Effectiveness, it will have a higher effectiveness than those who are considered typical users, called Typical Use Effectiveness. The only contraceptive method that is 100% effective is abstinence. Pregnancy is a possibility even if you are perfectly using contraceptive methods with high effectiveness. Unwanted pregnancies can be terminated through abortion.
Contraceptive Methods
It is important for sexual partners to discuss contraceptive options, asking question such as:
- Does either partner have allergies, such as a latex allergy?
- Are the partners concerned about transmission of sexually transmitted diseases?
- Can the female take hormonal birth control or are they contraindicated for them?
- Will it be challenging for the female to take a pill every day at the same time?
- Does either partner have religious beliefs that impact the use of contraception?
The answers to your questions may help in deciding which option to choose.
For example, couples who are concerned about STD’s need to choose contraceptive options that reduce the transmission of STD’s which means choosing to use either a male condom or female condom. Male condoms are much cheaper and easier to find than female condoms. It is important to understand that surgical, hormonal, or natural birth control options do not protect against STD’s. Couples who are in a long term committed relationship and are not concerned about STD’s and would like a long term contraceptive might choose a permanent surgical option or a long term option like an Intrauterine Device (IUD). Couples who have a latex allergy and still want to use condoms can choose lambskin or polyurethane condoms instead of the more commonly used latex condoms. Couples who are very concerned about unwanted pregnancies will want to choose a method with the highest effectiveness rate and ensure they use the method as perfectly as possible, they may also want to combine methods such as using birth control pills and condoms.
When choosing a contraceptive method it is important to understand the difference between surgical, hormonal, barrier, or fertility awareness methods.
- Surgical method (permanent option)
- Permanent methods of birth control that are also referred to as sterilization. These methods are for those who are sure that they do not want to conceive a child. Women choosing a permanent method can have their fallopian tubes tied or closed off, called a tubal ligation, or they can choose to have a small tube inserted into the fallopian tubes, called transcervical sterilization, which irritates the fallopian tubes causing scar tissue to form and close off the tubes. Men commonly get a vasectomy which is an outpatient procedure in which the tube that carries sperm is cut.
- Hormonal method (reversible)
- When a woman is pregnant they no longer release an egg each month and if there is no egg released, they cannot become pregnant. Hormonal methods reduce the chance of pregnancy by providing hormones to the woman that tricks the woman’s body into thinking they are pregnant, thus the egg is not released each month.
- Barrier method (reversible)
- In order for pregnancy to occur the egg from a woman and the sperm from a man must meet. If the sperm fertilizes the egg then conception, or pregnancy, occurs. Barrier methods of birth control work by creating a barrier in which the egg and sperm cannot meet.
- FAM: Fertility Awareness Method (reversible)
- In order for pregnancy to occur, the sperm from the male must meet the egg from the female. The egg from the female is typically released only one time per month, called ovulation, so the sperm has a limited time window to meet the egg. The FAM is based on avoiding sexual intercourse when it is most likely that the sperm and egg can meet. FAM must also take into consideration that sperm can live in a woman’s body up to 5 days.
| Name(s) | Type | Percentage of unwanted pregnancy within first year of typical use | Protect against STD’s? | Side effects and risks* *These are not all of the possible side effects and risks. Talk to your doctor or nurse for more information. |
How often you have to take or use
|
| Abstinence (no sexual contact) | Natural- reversible | Unknown (0 for perfect use) |
No | No medical side effects |
No action required, but it does take willpower. You may want to have a back-up birth control method, such as condoms.
|
| Female sterilization (tubal ligation, “getting your tubes tied”) | Surgical- permanent | Less than 1% | No | Pain, bleeding, risk of infection |
Surgery completed one time.
No action required after surgery
|
| Male sterilization (vasectomy) | Surgical- permanent | Less than 1% | No | Pain, bleeding, risk of infection |
Surgery completed one time. No action required after surgery
|
| Implantable rod (Implanon®, Nexplanon®) | Hormonal- reversible | Less than 1% | No | Headache, irregular periods, weight gain, sore breasts. Less common risk includes difficulty in removing the implant |
No action required for up to 3 years before removing or replacing
|
| Copper intrauterine device (IUD) (ParaGard®) | Nonhormonal- reversible | Less than 1% | No | Cramps for a few days after insertion. Missed periods, bleeding between periods, heavier periods. Less common but serious risks include pelvic inflammatory disease and the IUD being expelled from the uterus or going through the wall of the uterus. |
No action required for up to 10 years before removing or replacing
|
| Hormonal intrauterine devices (IUDs) (Liletta, Mirena®, and Skyla®) | Hormonal- reversible | Less than 1% | No | Irregular periods, lighter or missed periods. Ovarian cysts. Less common but serious risks include pelvic inflammatory disease and the IUD being expelled from the uterus or going through the wall of the uterus. |
No action required for 3 to 5 years, depending on the brand, before removing or replacing
|
| Shot/injection (Depo-Provera®) | Hormonal- reversible | 4-6% | No | Bleeding between periods, missed periods Weight gain Changes in mood Sore breasts Headaches Bone loss with long-term use (bone loss may be reversible once you stop using this type of birth control) |
Get a new shot every 3 months
|
| Oral contraceptives, combination hormones (“the pill” or “mini-pill)) | Hormonal- reversible | 7-9% | No | Headache, nasuea, sore breasts, changes in your period, changes in mood, weight gain, high blood pressure. Less common but serious risks include blood clots, stroke and heart attack; the risk is higher in smokers and women older than 35 |
Take at the same time every day
|
| Skin patch (Xulane®) |
Hormonal- reversible | 7-9% May be less effective in women weighing 198 pounds or more |
No | Skin irritation, headache, nasuea, sore breasts, changes in your period, changes in mood, weight gain, high blood pressure. Less common but serious risks include blood clots, stroke and heart attack; the risk is higher in smokers and women older than 35 |
Apply to skin for 21 days, remove for 7 days, replace with a new patch
|
| Vaginal ring (NuvaRing®) | Hormonal- reversible | 7-9% | No | Vaginal irritation and discharge, headache, nasuea, sore breasts, changes in your period, changes in mood, weight gain, high blood pressure. Less common but serious risks include blood clots, stroke and heart attack; the risk is higher in smokers and women older than 35 |
Insert into the vagina for 21 days, remove for 7 days, replace with a new ring
|
| Diaphragm with spermicide (Koromex®, Ortho-Diaphragm®) | Barrier- reversible | 12% | No | Irritation, allergic reactions, urinary tract infection (UTI), vaginal infections. Rarely, toxic shock if left in for more than 24 hours. Using a spermicide often might increase your risk of getting HIV. |
Insert into vagina before sexual intercourse. Remove after intercourse. Get refitted if you gain or lose weight or give birth
|
| Sponge with spermicide (Today Sponge®) | Barrier- reversible | 12-27% 12% for those who haven’t had a child, 27% for those who have given birth |
No | Irritation, allergic reactions, urinary tract infection (UTI), vaginal infections. Rarely, toxic shock if left in for more than 24 hours. Using a spermicide often might increase your risk of getting HIV. |
Insert into vagina before sexual intercourse. Remove after intercourse. |
| Cervical cap with spermicide (FemCap®) | Barrier- reversible | 17-29% | No | Irritation, allergic reactions, urinary tract infection (UTI), vaginal infections. Rarely, toxic shock if left in for more than 24 hours. Using a spermicide often might increase your risk of getting HIV. |
Insert into vagina before sexual intercourse. Remove after intercourse (up to 2 days after). |
| Male condom | Barrier- reversible | 13-18% | Yes | Condom may tear, break or slip off. Irritation or allergic reactions to latex condoms |
Put on penis before sexual intercourse. Use each time you have sex. Never use a male and female condom together.
|
| Female condom (“internal condom”) | Barrier- reversible | 21 | Yes | Condom may tear or slip out. Irritation or allergic reactions could occur. |
Insert into vagina or anus before sexual intercourse. Use each time you have sex. Never use a male and female condom together.
|
| Withdrawal — when a man takes his penis out of a woman’s vagina (or “pulls out”) before he ejaculates (has an orgasm or “comes”) | Natural- reversible | 22 | No | Sperm can be released before the man pulls out, putting you at risk for pregnancy. |
Use each time you have sex
|
| Fertility Awareness Method: Calendar, temperature, or rhythm method | Natural- reversible | 24 | No | Can be hard to know the days you are most fertile (when you need to avoid having sex or use back-up birth control) |
Depending on method used, takes planning each month
|
| Spermicide alone | Barrier- reversible | 28 Works best if used along with a barrier method, such as a diaphragm |
No | Irritation, allergic reactions, urinary tract infection (UTI), vaginal infections. Using a spermicide often might increase your risk of getting HIV. |
Use each time you have sex
|
Abortion and Roe v. Wade
“Jane Roe,” a woman who wanted to safely and legally end her pregnancy, challenged a Texas statute that made it a crime to perform an abortion unless the woman’s life was in danger. In the ruling, the U.S. Supreme Court recognized for the first time that the constitutional right to privacy “is broad enough to encompass a woman’s decision whether or not to terminate her pregnancy” (Roe v. Wade, 1973). Roe v. Wade has come to be known as the case that legalized abortion nationwide. On June 24, 2022, after upholding this constitutional right for nearly 50 years, the U.S. Supreme Court ruled that “the Constitution does not confer a right to abortion,” thus voted to reverse their decision, leaving the ability to have an abortion to state law. It is estimated that about half of the states in America will either completely ban, or severely reduce, access to a legal and safe abortion.
There is no way to know how many women died receiving illegal abortions prior to the legalization of abortion in 1973. However, since the early 20th century, researchers, scientists, and doctors have attempted to estimate the number of illegal abortions performed and the corresponding death rate. Some estimates state that it could have been as low as 200,000 illegal abortions to 1.2 million illegal abortions performed each year causing as many as 5,000 to 10,000 annual deaths.
Although we do not know exactly how many deaths occured prior to the legalization of abortion in 1973, we do know that after 1973 when abortions were legal they were very safe causing less than 1 death per 100,000 people. Legal abortions are so safe that in 2018 there were only two deaths total from complications of an abortion. Thus, the death rate before 1973 and after were very likely dramatically different. The rate of complication for abortion is less than childbirth itself, and even lower than wisdom teeth removal.
Legal abortions in the U.S. are not only safe, but also very common. In the US, in 2019, there were 195 abortions per 1,000 live births, meaning about one out of every five pregnancies was terminated through abortion[7]. In 2019, the majority of abortions occurred early in gestation (≤9 weeks), when the risks for complications are lowest. In addition, over the past 10 years, the number of abortions performed ≤9 weeks’ gestation increased from 74.8% in 2010 to 77.4% in 2019. Abortion can be completed with medication or by a procedure which is often called surgical abortion or aspiration abortion.
A committee of the National Academies of Sciences, Engineering, and Medicine reviewed the data available and confirmed in their report in 2018 that all forms of abortion including medication and aspiration abortion are safe and effective and that the only factors decreasing safety are those decreasing access[8][9]. A medication abortion can be completed at home, is non-invasive, and can be done up to 11 weeks, whereas an aspiration abortion is performed in a hospital or clinic and can be done up to 16 weeks.
It will be years before data is available to understand how the U.S. Supreme Court’s decision to overturn the constitutional right to an abortion may impact women’s health across the U.S., especially on a state-by-state basis where access may lead to health disparities.
Key Takeaways for Chapter
- Social wellness is an important part of overall wellness.
- Love is difficult to define.
- Sternberg defines love as including varying levels of intimacy, passion, and commitment.
- A person own “love story” may impact their own relationships.
- It is important to understand the differences between healthy and unhealthy relationships.
- Effective communication includes being assertive and using “I” statements.
- Sex and Gender mean two different things.
- Pregnancy occurs when a females egg is fertilized by a males sperm, this is called conception.
- Various contraceptive methods are available that can help to reduce the chances of pregnancy and STD transmission.
- Abortion is the act of ending a pregnancy.
Media Attributions
- Triangular Theory of Love © en:User:Lnesaderivative work: Rafy, Public domain, via Wikimedia Commons is licensed under a Public Domain license
- Holt-Lunstad J, Smith TB, Layton JB (2010) Social Relationships and Mortality Risk: A Meta-analytic Review. PLoS Med 7(7): e1000316. https://doi.org/10.1371/journal.pmed.1000316 ↵
- Howick, J., Kelly, P., & Kelly, M. (2019). Establishing a causal link between social relationships and health using the Bradford Hill Guidelines. SSM - population health, 8, 100402. https://doi.org/10.1016/j.ssmph.2019.100402 ↵
- Sternberg, R. (n.d.). Love. Robert J. Sternberg. http://www.robertjsternberg.com/love ↵
- Sternberg, R. (2022, January 20). Sternberg's theory of love as a story. The Love Multiverse. https://lovemultiverse.com/understanding-love/different-kinds-of-love-stories/#kinds-of-stories ↵
- Sternberg, R. J., Hojjat, M., & Barnes, M. L. (2001). Empirical tests of aspects of a theory of love as a story. European Journal of Personality, 15(3), 199–218. https://doi.org/10.1002/per.405 ↵
- Characteristics of Healthy & Unhealthy Relationships | Youth.gov. (n.d.). Youth.Gov. https://youth.gov/youth-topics/teen-dating-violence/characteristics ↵
- Kortsmit K, Mandel MG, Reeves JA, et al. Abortion Surveillance — United States, 2019. MMWR Surveill Summ 2021;70(No. SS-9):1–29. DOI: http://dx.doi.org/10.15585/mmwr.ss7009a1 ↵
- Upadhyay UD, Desai S, Zlidar V, Weitz TA, Grossman D, Anderson P, Taylor D. Incidence of emergency department visits and complications after abortion. Obstet Gynecol. 2015 Jan;125(1):175-183 ↵
- White K, Carroll E, Grossman D. Complications from first-trimester aspiration abortion: a systematic review of the literature. Contraception. 2015 Nov;92(5):422-38. ↵

{kind=link}