This section uses text and an image to define and compare the Medical Model approach to disability (which locates disability as a problem in the individual) from the Social and Human Rights Model approaches to disability (which locate disablement as a problem in the environment).
If you prefer learning visually, you may like to scroll down to the end of this page to view the image first.
The Medical Model Approach to Disability
Historically, Western societies have viewed disability as a deficiency residing in a person’s body and/or mind. From this perspective:
- Disability is seen as something abnormal, bad, pathological, problematic, and as something that needs to be fixed, cured, removed, hidden, or minimized.
- Non-disabled bodies are seen as “normal”, healthy, better, and good.
This leads to the poor treatment of disabled people, who are often devalued and disrespected and pushed out of our communities. These sorts of perspectives, treatments, and impacts are typically referred to as a Medical Model Approach to disability.
A significant limitation of a Medical Model Approach is that it can be so focused on identifying “defects” within the individual that it fails to pay attention to significant problems in our society and the role of our physical, social, and attitudinal environments in either producing barriers or promoting accessibility and inclusion.
Furthermore, when we get too focused on “fixing” individual bodies, we can forget that legislation affirms the inherent dignity, worth, and human rights of disabled people. People with disabilities do not need to “change” in order to access their human rights, and they deserve to make their own decisions about their bodies and lives, just like anyone else (Withers, 2012, n.p.).
The Social and Human Rights Model Approaches to Disability
The Social Model and the Human Rights Model are two approaches to disability that emphasize structural barriers in society, as well as disabled people’s rights to be included and treated fairly. Accessible Education, and this FLEX Forward resource, view disability from these perspectives.
| Social Model | Human Rights Model | |
| Core Values | There is natural and valuable variation and difference among human beings. | All human beings, including people with disabilities, deserve respect and have human and legal rights protected by law that must be upheld. |
| Framing the “Problem” | People with disabilities are not, and should not be treated like, a problem.
The problem is exclusionary structures, policies, attitudes, and environments that have not been designed with a diverse collective of people in mind. While a person may experience an impairment or difference, the person is more “disabled” by barriers in society than by any individual trait. |
The problem is discrimination.
Discriminating against people with disabilities is illegal. |
| Vision for Change | The Social Model aims to identify and remove physical, communication, technological, organizational/systemic, and attitudinal barriers. | The Rights Model emphasizes the rights that students, staff, and faculty with disabilities have in any educational or employment environment.
This includes the rights to:
|
| Actions | Approaching disability on campus through a Social Model would have us:
|
Approaching disability on campus through a Rights Model would have us:
|
*Chart adapted from Council of Ontario Universities (2017a).
Comparing Different Approaches to Disability
The image below depicts the difference between Medical Model approaches that locate the “problem” of disability in the individual person, and Social and Human Rights Model approaches that locate the “problem” in external barriers.
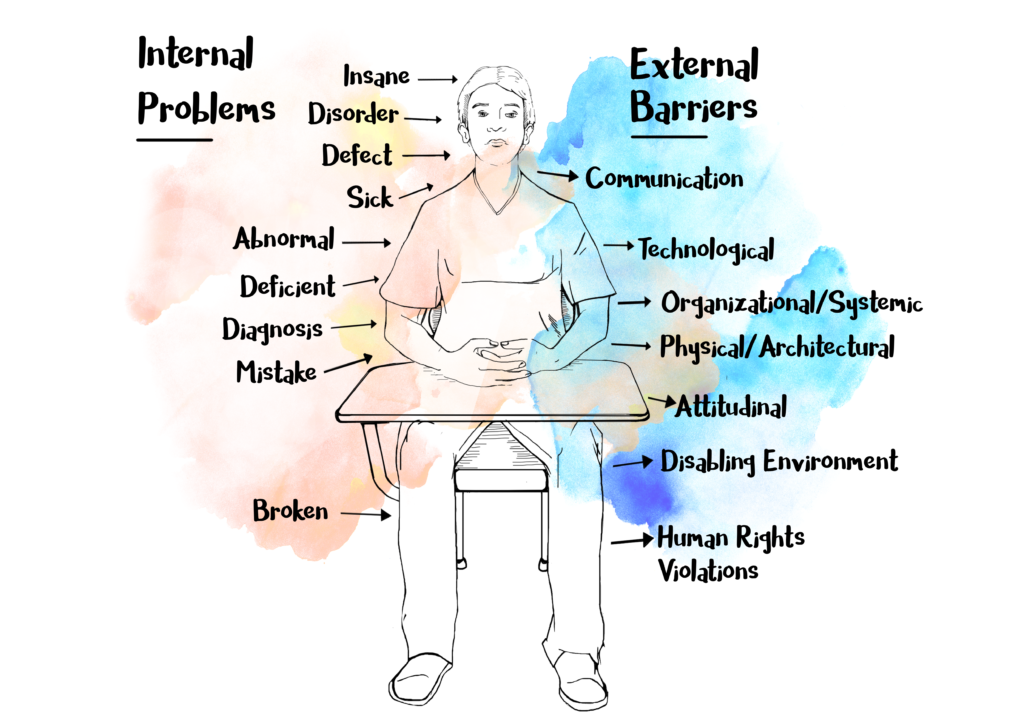
This chart offers some examples of external barriers that can exclude and disable people. The Social and Human Rights Models of disability, and this FLEX Forward resource, work to anticipate and mediate these and other types of barriers.
| Type of Barrier | Examples |
| Physical or Architectural Barriers | Stairs, poor sound quality, lack of accessible or all gender washrooms |
| Information or Communication Barriers | Heavy use of academic jargon in the classroom without clarification or definition, speaking too quickly |
| Technological Barriers | Documents incompatible with screen-readers , lack of availability of TeleTypewriters (TTY) for typing communication by phone rather than speaking |
| Organizational or Systemic Barriers | Tuition fees that require students to take out substantial student loans, unclear learning objectives, rigid class attendance and participation requirements |
| Attitudinal Barriers | Pathologizing attitudes that see disabled students, staff, and faculty as less capable or qualified to participate in university |
*Chart adapted from Council of Ontario Universities (2017b)
