7
Case
Age: 25-year-old man
Reason for referral to ophthalmology: Vision loss in the left eye
Past medical history: None
Past ocular history: None
Medications: None
Habits: Non-smoker and drinks alcohol socially
HPI: Five days ago, he woke up with vision loss in his left eye. He went to an urgent care center and was referred to ophthalmology. He denies eye pain or pain with eye movements. He has felt fatigued, tired, and developed a low-grade fever over the past few days.
Ophthalmological Examination:
Blood pressure: 125/80, heart rate 77
Visual acuity is 20/20 OD, counting fingers OS
Pupils are equal sizes and there is a left RAPD
Color vision is 14/14 OD and 0/14 OS correct Ishihara color plates
Ocular motility and alignment are normal
Slit lamp examination is normal. There is 1/2+ cells in the vitreous in the left eye.
Neurological examination is normal
1. This patient’s examination is atypical for optic neuritis because there is:
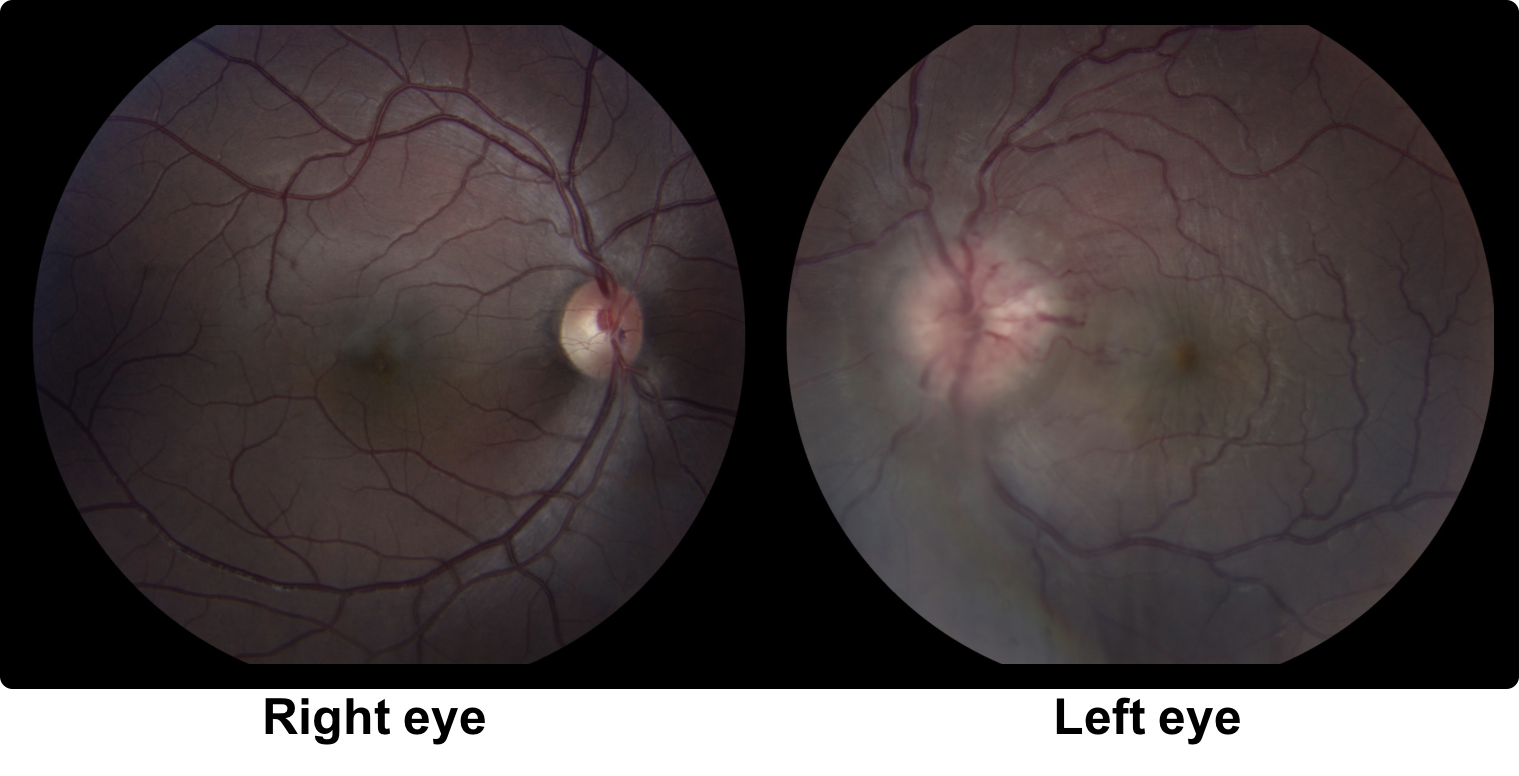
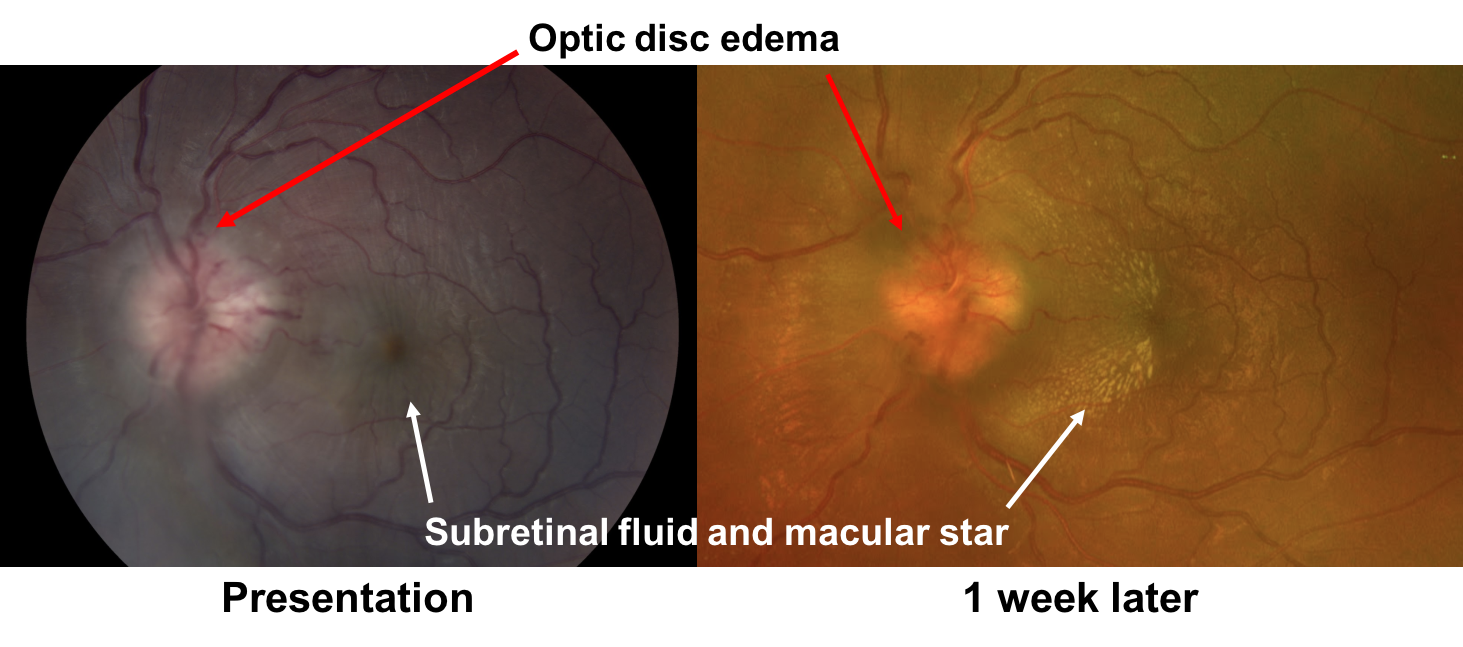
- Mild optic disc edema in the left eye
- Bilateral optic disc edema
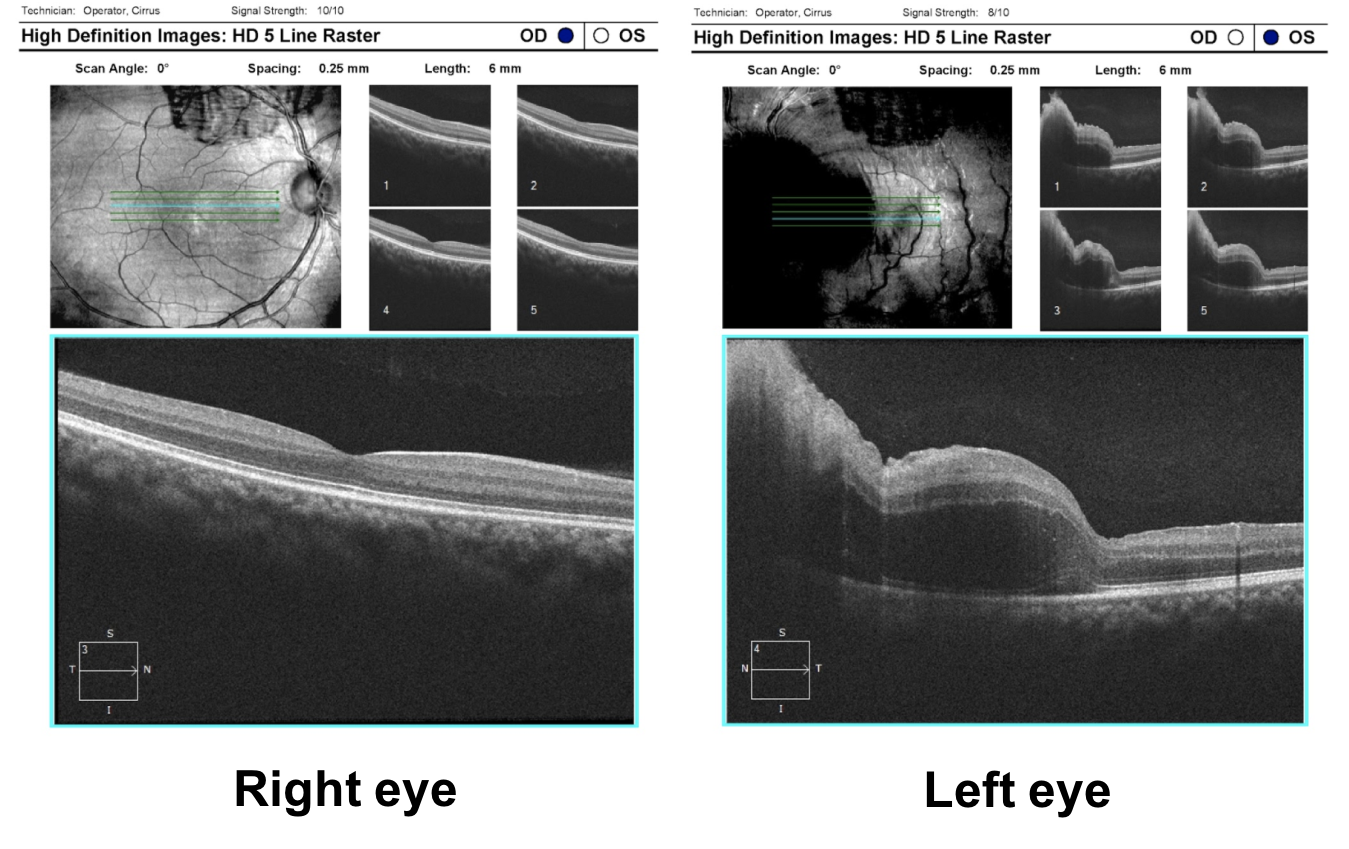
- Significant optic disc edema and subretinal fluid in the macula in the left eye
- Tortuous retinal vessels in the left eye
1. This patient’s examination is atypical for optic neuritis because there is: 3. Significant optic disc edema and subretinal fluid in the macula in the left eye.
In optic neuritis, there is typically mild optic disc edema or the optic nerve appears normal. The presence of significant optic disc edema with macular edema or subretinal fluid should lead to the consideration of other diagnoses.
2. Which of the following is the most likely diagnosis?
- Central serous retinopathy
- Posterior scleritis
- Neuroretinitis
- Anterior uveitis
2. Which of the following is the most likely diagnosis? 3. Neuroretinitis
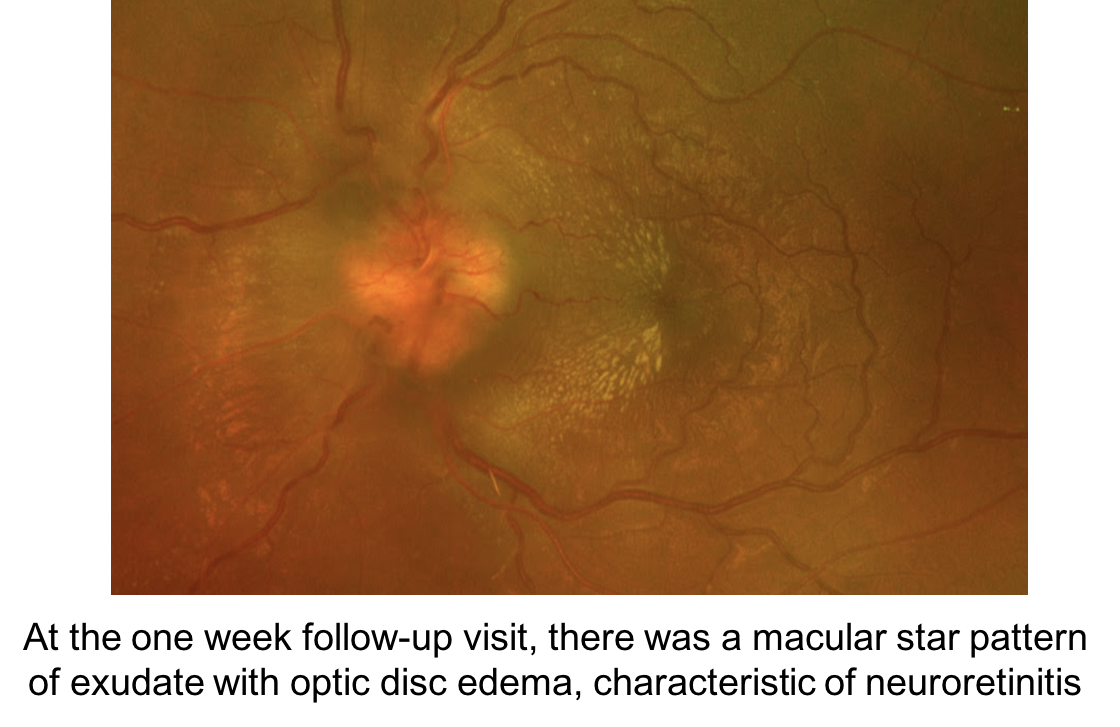
Neuroretinitis is characterized by inflammation of the optic disc vasculature leading to optic disc edema and macular star formation. Leakage from the optic disc leads to accumulation of lipid-rich fluid in the outer plexiform layer, giving the typical macular star appearance. The optic disc edema precedes the macular star, which is usually a later finding. A follow-up fundus photograph from the same patient is shown below.
3. What conditions can cause optic disc edema and a macular star?
- Hypertensive retinopathy
- Non-arteritic anterior ischemic optic neuropathy
- Papilledema
- Optic disc and juxtapapillary tumors
- All of the above
3. What conditions can cause optic disc edema and a macular star? 5. All of the above
In addition to neuroretinitis, other conditions may cause optic disc edema with a macular star. It is important to consider these entities in the differential diagnosis, which is summarized below.
Clinical Pearl
Causes of optic disc edema with a macular star include:
- Neuroretinitis
- Hypertensive retinopathy
- Papilledema
- Anterior ischemic optic neuropathy
- Disc and juxtapapillary tumors (angioma, melanoma)
4. What questions are important to ask on history in this patient?
- Presence of fever and flu-like symptoms
- Close proximity to a cat
- Recent tick bites
- Exposure to tuberculosis
- All of the above
4. What questions are important to ask on history in this patient? 5. All of the above
The differential diagnosis of neuroretinitis includes infectious and noninfectious entities. It is important to perform a thorough history and review of systems in these cases. The differential diagnosis of neuroretinitis is summarized below.
Clinical Pearl
The differential diagnosis for neuroretinitis includes:
Infectious:
- Bacteria: Bartonella henselae, Rocky Mountain spotted fever, tuberculosis, salmonella
- Protozoa: Toxoplasmosis
- Spirochete: Syphilis, Lyme, leptospirosis
- Virus: Measles, mumps, rubella, herpes zoster, herpes simplex, cytomegalovirus, Epstein-Barr, coxsackie B, chikungunya
- Nematode: Toxocara canis, Baylisascaris procyonis
- Fungus: Histoplasmosis, actinomycosis, coccidiomycosis
Noninfectious:
- Sarcoidosis, inflammatory bowel disease, polyarteritis nodosa, IRVAN (idiopathic retinal vasculitis and neuroretinitis), TINU (tubulointerstitial nephritis and uveitis)
5. What is the most common cause of infectious neuroretinitis?
- Lyme disease
- Tuberculosis
- Syphilis
- Bartonella henselae
5. What is the most common cause of infectious neuroretinitis? 4. Bartonella henselae
Bartonella henselae is the principal etiologic agent of cat scratch disease and the most common infectious cause of neuroretinitis. It is a slow-growing, gram-negative bacterium. A published review of the literature found that the average age of onset of cat scratch neuroretinitis was 24.5 years (range 4 to 64) and systemic symptoms were reported in 73% of patients. These usually precede the ocular manifestations and include mild to moderate flu-like symptoms associated with regional adenopathy. In a minority of cases, the organisms can disseminate and infect the liver, spleen, and central nervous system and result in life-threatening complications.
6. How can Bartonella henselae be transmitted?
- Only by the scratch of a cat that produces visible blood
- Contact with cat saliva on mucosal surfaces or through broken skin
- Sexually transmitted by humans
- Respiratory secretions from an infected human
6. How can Bartonella henselae be transmitted? 2. Contact with cat saliva on mucosal surfaces or through broken skin
There is strong evidence linking Bartonella henselae infection to cat exposure, particularly kittens and cats with fleas. Transmission to humans may occur after a scratch or bite from an infected cat, contact with cat saliva on mucosal surfaces or broken skin, and rare cases have been reported after exposure to dogs, which was likely a result of flea bites. Fleas play an important role in cat-to-cat transmission and flea infestation has been reported as the risk factor most associated with seroconversion among cats.
7. Which of the following is true regarding serologic testing for cat scratch disease?
- A negative serologic test rules out the disease
- Titers greater than 1:256 strongly suggest active or recent infection
- A positive IgM test indicates chronic disease
- Cerebrospinal fluid is preferable to serology for patients with neuroretinitis
7. Which of the following is true regarding serologic testing for cat scratch disease? 2. Titers greater than 1:256 strongly suggest active or recent infection
A diagnosis of cat scratch neuroretinitis in patients with characteristic clinical features can be confirmed with serologic testing, which is usually performed with an indirect fluorescence assay. A positive IgM test strongly suggests active disease or very recent infection and the IgG titers are very important (see Clinical Pearl below). Negative serologic testing does not rule out the disease and the production of IgM can be very brief, resulting in negative testing. Repeat serology testing in 2 weeks can be performed if there is a high index of suspicion since the initial testing may have been performed after the IgM has returned to normal, but before the IgG titers have risen.The IgG titer usually remains high for 2 or more years after the onset of symptoms.
Other approaches used to support the diagnosis of cat scratch disease include culture, histopathologic examination of the primary inoculation site, polymerase chain reaction (PCR) or skin testing. Bartonella is a notoriously slow-growing bacterium and the microbiology lab should be informed about this potential diagnosis so they can optimize the culture techniques and extend the incubation period. PCR testing of aqueous fluid may be tested since blood has a very low sensitivity and is not recommended. Histopathologic testing is not considered definitive, but may show dermal necrosis with surrounding histiocytes and epitheliod cells or the bacilli may be seen with Warthin-Starry stain.
Clinical Pearl
Bartonella IgG titers:
- < 1:64: the patient does not have current Bartonella infection
- 1:64-1:256: possible Bartonella infection
- > 1:256: strongly suggests active or recent infection.
8. Which of the following is true regarding the treatment of cat scratch neuroretinitis?
- Most patients have gradual resolution of symptoms without treatment
- A prospective randomized trial found doxycycline 100 mg PO twice daily with rifampin 300 mg PO twice daily for 4 to 6 weeks resulted in improved visual outcomes
- Prednisone should be initiated in all cases to prevent permanent vision loss
- All of the above
8. Which of the following is true regarding the treatment of cat scratch neuroretinitis? 1. Most patients have gradual resolution of symptoms without treatment
There is limited evidence for the treatment of patients with cat scratch neuroretinitis and most patients have gradual resolution of symptoms even without treatment. There is evidence supporting the use of azithromycin in the treatment of patients with lymphadenitis who were randomized to receive azithromycin or placebo. At 1 month follow-up, there was an 80% decrease in lymph node volume in 50% of the azithromycin treated patients compared to only 7% of the placebo group. There are no prospective studies on patients with cat scratch neuroretinitis. A small, uncontrolled, retrospective study of 7 patients treated with doxycycline 100 mg twice daily and rifampin 300 mg twice daily for 4 to 6 weeks appeared to be beneficial compared to historical controls. The use of steroids is based on expert opinion and are usually reserved for patients with persistent or severe disease. There is no consensus on the optimal treatment, if any, for cat scratch neuroretinitis, but treatment should certainly be considered for immunocompromised patients and those with significant vision loss or prominent systemic symptoms.
Clinical Pearl
Proposed antibiotic regimens for cat scratch disease include:
- Azithromycin 500 mg for 1 day followed by 250 mg daily for 4 days
- Doxycycline 100 mg twice daily with rifampin 300 mg twice daily for 4 to 6 weeks
- Bactrim or Septra DS twice daily for 7 to 10 days
- Ciprofloxacin 500 mg twice daily for 7 to 10 days
9. What do you expect to see on this patient’s MRI of the orbits with contrast?
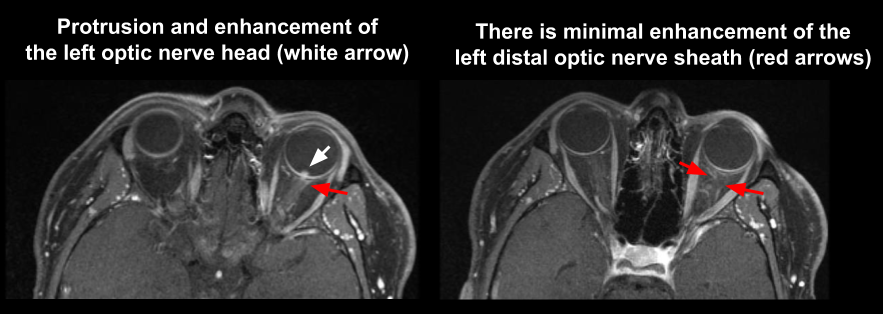
- Enhancement of the left optic nerve from the optic chiasm to just behind the globe
- Enhancement of the left intracranial optic nerve
- Enhancement of the left intracanalicular optic nerve
- No significant enhancement of the intraorbital, intracanalicular or intracranial optic nerve
9. What do you expect to see on this patient’s MRI of the orbits with contrast? 4. No significant enhancement of the intraorbital, intracanalicular or intracranial optic nerve
10. His MRI of the brain was normal. What is his 15-year risk of multiple sclerosis?
- No increased risk
- 15%
- 25%
- 40%
10. His MRI of the brain was normal. What is his 15-year risk of multiple sclerosis? 1. No increased risk
11. This patient was tested for syphilis and a serum nontreponemal test was used. Which of the following is true regarding nontreponemal testing for syphilis?
- They are based on reactivity of serum with a cardiolipin-cholesterol-lecithin antigen
- They include rapid plasma reagin (RPR) and Venereal Disease Research Laboratory (VDRL)
- False positive testing can be seen in the setting of autoimmune disease, other infections and malignancy
- False negative testing may be seen when the antibody concentration is very high
- All of the above
11. This patient was tested for syphilis and a serum nontreponemal test was used. Which of the following is true regarding nontreponemal testing for syphilis? 5. All of the above
- They are qualitative only (reported as reactive or nonreactive)
- Treponemal testing becomes nonreactive after an appropriate treatment course
- They do not detect other related spirochete species
- They have been traditionally used as screening tests for syphilis
12. Which of the following is true regarding treponemal testing for syphilis? 1. They are qualitative only (reported as reactive or nonreactive)
Treponemal tests detect the presence of antibodies (IgM or IgG) against T. Pallidum specific proteins, which are generated within 3 weeks of infection. These tests include Fluorescent treponemal antibody absorption (FTA-ABS), microhemagglutination test for antibodies to T. pallidum (MHA-TP), T. pallidum particle agglutination assay (TPPA), T. pallidum enzyme immunoassay (TP-EIA). Traditionally, these tests were used to confirm the infection after nontreponemal tests are reactive since they are more complex and expensive to perform. However, newer, automated testing algorithms have led to an increasing use of treponemal tests as initial screening. Once they are positive, they usually remain positive for life and must be used in conjunction with nontreponemal tests, which decline with successful treatment. Due to a similar antigen profile with other spirochete subspecies, false positive tests may be seen with other non-venereal diseases such as yaws, pinta, and bejel.
Clinical Pearl
Treponemal tests remain positive for life after even after treatment for syphilis.
13. This patient was tested for tuberculosis using Quantiferon-TB Gold testing. Which of the following is true regarding this test?
- Release of interferon-gamma is measured after stimulation with antigens derived from Mycobacterium tuberculosis
- Active and latent infection can be differentiated
- Results are affected by Bacille Calmette-Guérin (BCG) vaccination
- Nontuberculous mycobacteria often result in false-positive results
- All of the above
13. This patient was tested for tuberculosis using Quantiferon-TB Gold testing. Which of the following is true regarding this test? 1. Release of interferon-gamma is measured after stimulation with antigens derived from Mycobacterium tuberculosis
Interferon-gamma release assays such as Quantiferon-TB Gold are in vitro tests that measure T-cell release of interferon-gamma after stimulation with Mycobacterium tuberculosis antigens. This is based on the principle that mononuclear cells in individuals infected with tuberculosis will release more interferon-gamma than healthy controls. However, since it is a surrogate marker of a cellular immune response, it cannot differentiate between active and latent infection. Unlike the tuberculosis skin test, it is not affected by BCG vaccine and it is largely unaffected by nontuberculous myocobacterium. Test results typically take 24 to 48 hours to obtain.
14. Which of the following is true regarding the clinical manifestations of Lyme disease?
- All patients with early disseminated or late Lyme disease give a history of the characteristic skin lesion (erythema migrans)
- Erythema migrans is characterized by concentric erythematous rings
- Intermittent or persistent arthritis is common within the first days to weeks after the tick bite
- There are very characteristic systemic symptoms early in the disease course allowing for easy recognition
14. Which of the following is true regarding the clinical manifestations of Lyme disease? 2. Erythema migrans is characterized by concentric erythematous rings
Lyme disease is a tick-borne illness caused by three pathogenic spriochete species, most commonly, Borrelia burgdorferi in North America. The clinical manifestations of Lyme disease can be categorized into early localized disease (few days to one month after the tick bite), early disseminated disease (weeks to months after the tick bite), and late or chronic disease (months to years after the tick bite). Erythema migrans is the characteristic skin lesion seen in the early phase of the disease in about 80% of patients and is characterized by concentric erythematous rings. The characteristic symptoms of Lyme disease by each stage are summarized below.
Clinical Pearl
Clinical manifestations of Lyme disease:
- Early localized disease (few days to one month after the tick bite)
- Erythema migrans (seen in about 80% of patients)
- Nonspecific systemic symptoms: fatigue, malaise, myalgias, arthralgias, regional lymphadenopathy
- Early disseminated disease (weeks to months after the tick bite)
- Neurologic disease: cranial neuropathy (most commonly facial nerve), peripheral neuropathy, meningitis
- Eye involvement: neuroretinitis, uveitis, conjunctivitis
- Carditis: conduction block, myopericarditis
- Liver disease: liver enzyme abnormalities, hepatitis
- Kidney disease: microhematuria, proteinuria
- Musculoskeletal: migratory arthralgias
- Lymphadenopathy: regional or generalized
- Late or chronic disease (months to years after the tick bite)
- Muskuloskeletal symptoms: intermittent monoarticular or oligoarticular arthritis, persistent monoarthritis
- Neurologic: peripheral neuropathy, encehalomyelitis
15. Which of the following is true regarding serologic testing for Lyme disease?
- It should be performed in all patients who have erythema migrans and a history supportive of Lyme disease
- It is recommended in all asymptomatic patients living in a Lyme endemic area
- It should be used to rule out Lyme disease in patients with only nonspecific symptoms such as fatigue and malaise
- A two-tiered system that includes a sensitive enzyme immunoassay and a Western blot test is typically used
- All of the above
15. Which of the following is true regarding serologic testing for Lyme disease? 4. A two-tiered system that includes a sensitive enzyme immunoassay and a Western blot test is typically used
Serologic testing is an important tool in the diagnosis of Lyme disease, but must be performed in the right clinical context. There is no need to perform serologic testing in patients with erythema migrans and recent travel to a Lyme endemic area since they should be treated for the disease given the high clinical suspicion. Serologic testing should not be used to screen asymptomatic patients in a Lyme endemic area or be used in patients with only non-specific symptoms since there is a greater chance of false-positive than true positive results. In patients that reside or travelled to a Lyme endemic area, have a risk factor for tick exposure, and have symptoms consistent with early disseminated or late disease, a two-tiered testing algorithm is used. First, a sensitive enzyme immunoassay such as ELISA is used and if this is negative, no further testing is required. If there is an equivocal or positive ELISA test, Western blotting is performed. A negative Western blot supercedes the ELISA test and the patient is considered negative for Lyme whereas a positive test is considered confirmatory of infection with Borrelia burgdorferi.
16. Which of the following is true regarding the treatment of early disseminated Lyme disease?
- Azithromycin is recommended as first-line therapy
- Doxycycline is an effective oral agent with good penetration into the central nervous system
- Doxycycline can be used in young children or pregnant women
- Intravenous antibiotics, particularly ceftriaxone, has been shown to be superior to oral antimicrobials
- All of the above
16. Which of the following is true regarding the treatment of early disseminated Lyme disease? 2. Doxycycline is an effective oral agent with good penetration into the central nervous system
Based on the results of clinical trials, amoxicillin, doxycycline or cefuroxime are considered to have equivalent efficacy. An open-label controlled trial demonstrated a similar clinical cure rate among patients with early disseminated disease randomized to doxycyline 100 mg twice daily for 21 days or cetriaxone 2 g daily intravenously or intramuscularly for 14 days. Doxycycline has good penetration into the central nervous system, but is not recommended for children under 8 years of age or pregnant or lactating women due to the risk of tooth staining or dental enamel hypoplasia.
Case Summary
He developed left eye vision loss and felt more fatigued with a low-grade fever. He recently got two new pet kittens. His examination revealed significant left optic disc edema and subretinal fluid and serologic testing confirmed cat scratch disease. He was treated with Bactrim DS for 10 days and at his follow-up appointment a macular star was evident. His vision improved and at a 3 month follow-up appointment, his visual function was normal.
Further reading:
- Purvin V, Sundaram S, Kawasaki A. Neuroretinitis: review of the literature and new observations. J Neuroophthalmol 2011;31(1):58-68. https://www.ncbi.nlm.nih.gov/pubmed/21317731
- Bhatti MT, Lee MS. Should patients with bartonella neuroretinitis receive treatment? J Neuroophthalmol 2014;34(4):412-416. https://www.ncbi.nlm.nih.gov/pubmed/25405664
- Gulati A, Yalamanchili S, Golnik KC, Lee AG. Cat scratch neuroretinitis: the role of acute and convalescent titers for diagnosis. J Neuroophthalmol 2012;32(3):243-245. https://www.ncbi.nlm.nih.gov/pubmed/21941214
- Soreng K, Levy R, Fakile Y. Serologic testing for syphilis: benefits and challenges of a reverse algorithm. Clin Microbiol Newsl 2014;36(24):195-202. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5568569/
- Dattwyler RJ, Luft BJ, Kunkel MJ, et al. Ceftriaxone compared with doxycyline for the treatment of acute disseminated Lyme disease. N Engl J Med 1997; 337:289-295. https://www.ncbi.nlm.nih.gov/pubmed/9233865
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and Babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2006;43(9):1089-1134. https://academic.oup.com/cid/article/43/9/1089/422463