3
Case
Age: 63-year-old white man
Reason for referral to ophthalmology: Sudden vision loss in the right eye
Past medical history: Hypertension, type 2 diabetes, dyslipidemia, obstructive sleep apnea
Past ocular history: Cataract surgery with posterior chamber intraocular lens 3 years ago in both eyes
Medications: Hydrochlorothiazide, valsartan, atorvastatin, metformin
Habits: Non-smoker and does not drink alcohol
History of Present Illness (HPI): Five days ago, he suddenly lost vision in the inferior part of the visual field in his right eye. It did not improve after he woke up the next day and he went to the emergency room (ER) for an evaluation. A detailed review of systems was performed and was negative. A CT scan of the head without contrast and an EKG were performed and were normal. An ophthalmology consultation was requested.
Ophthalmological examination:
Blood pressure: 143/86, heart rate 86
Visual acuity is 20/40 OD, 20/20 OS
Pupils are equal sizes and reactive to light, there is a right RAPD
Color vision is 14/14 correct Ishihara plates in both eyes
Ocular motility and alignment are normal
Slit lamp examination is normal
Neurological examination is normal 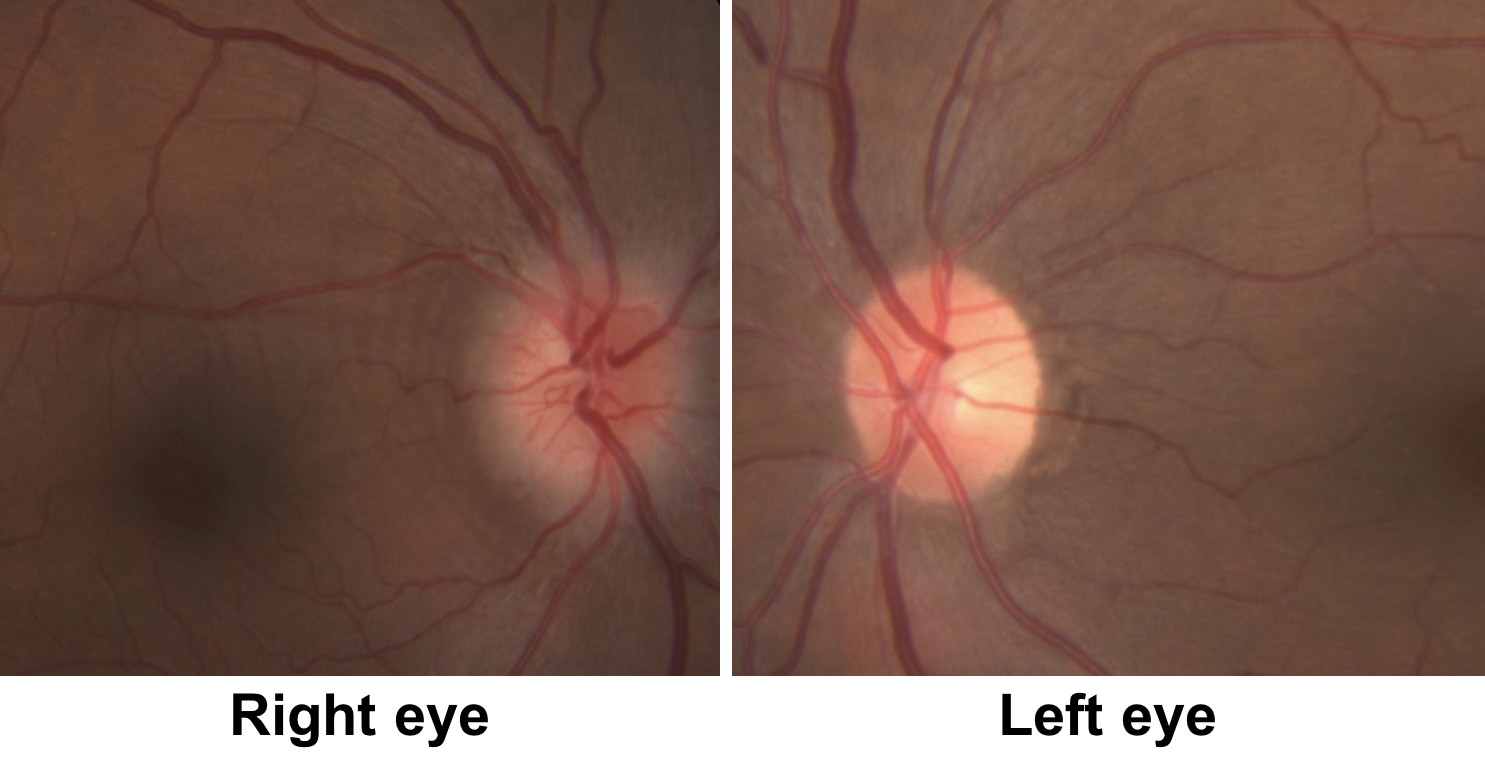
1. Which of the following is the best description of the patient’s right optic nerve?
- Normal appearance
- Optic disc edema and peripapillary wrinkles
- Optic disc pallor
- Optic disc drusen
1. Which of the following is the best description of the patient’s right optic nerve? 2. Optic disc edema and peripapillary wrinkles
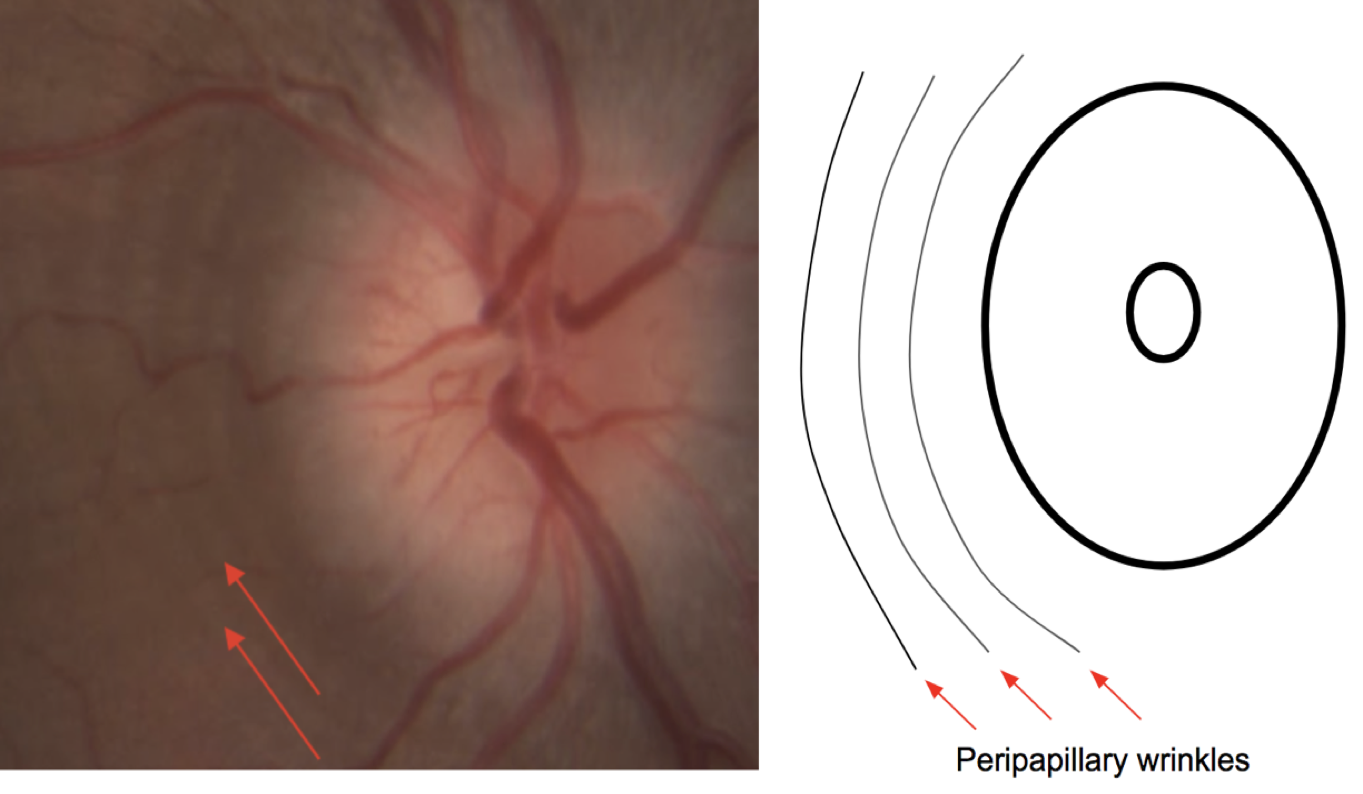
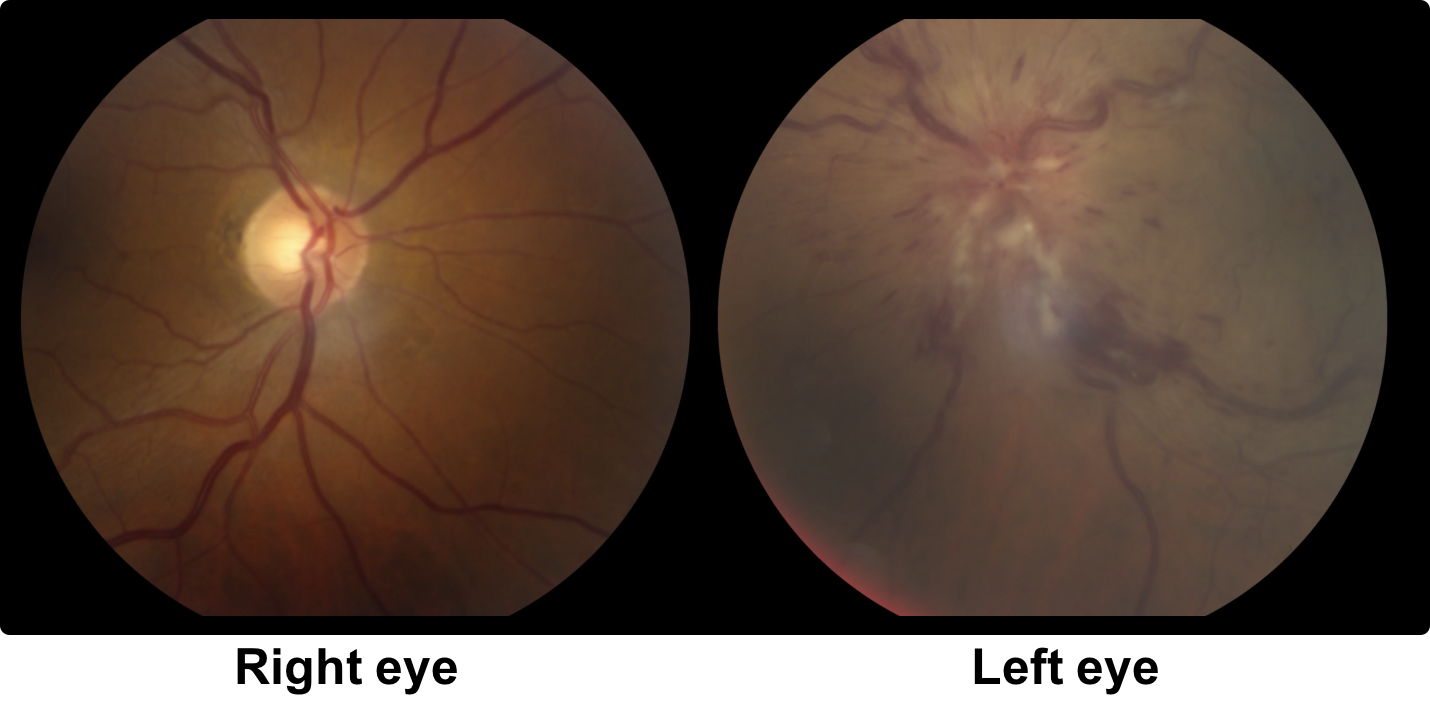
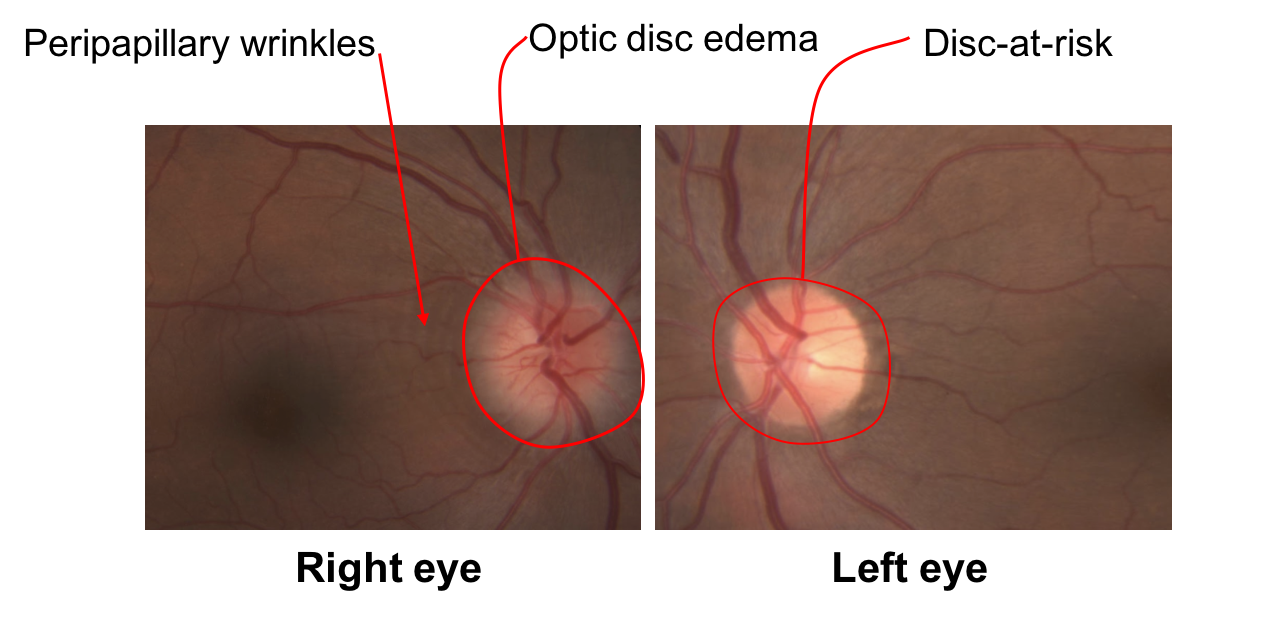
The right optic disc is hyperemic with a mild to moderate amount of edema as evidenced by blurring of the disc margins. Peripapillary wrinkles can also be seen (red arrows), which are caused by displacement of the retina by the disc edema leading to the formation of a series of concentric folds. Peripapillary wrinkles may be seen in optic neuropathies with optic disc edema or in papilledema (also known as Paton’s lines).
2. What is the best description of the left optic nerve?
- Disc-at-risk
- Optic disc edema
- Optic disc pallor
- Optic disc drusen
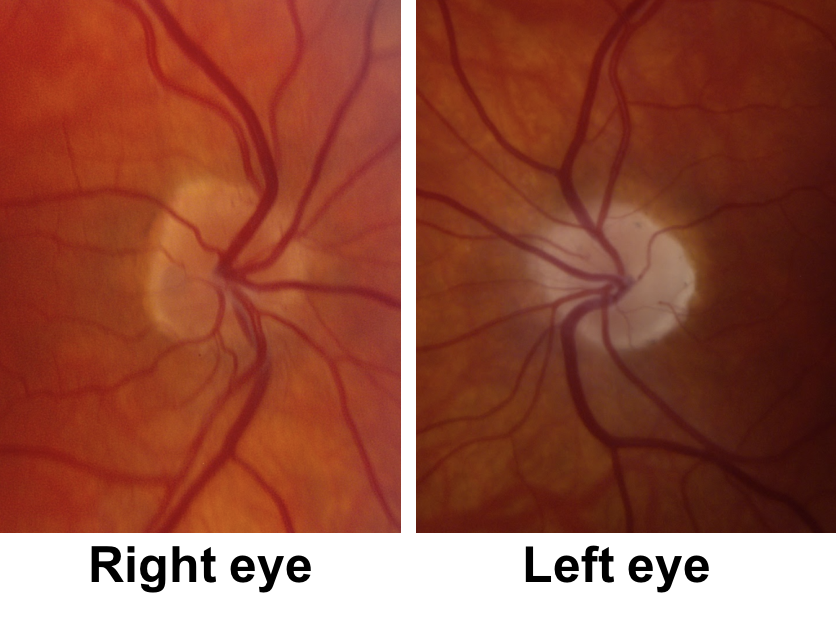
2. What is the best description of the left optic nerve? 1. Disc-at-risk
The left eye has a “disc-at-risk”, meaning there is a relatively crowded optic nerve head with a small or absent physiologic cup (usually a cup-to-disc ratio < 0.2). The left disc-at-risk suggests that the right eye had a similar appearance before the onset of optic disc edema.
Clinical Pearl
A disc-at-risk is essential for the diagnosis of non-arteritic anterior ischemic optic neuropathy (NAION).
The cup-to-disc ratio of the fellow eye is used as a marker of what the affected optic nerve appeared like before the onset of disc edema.
3. What medication may have predisposed the patient to developing his current condition?
- Ethambutol
- Oral steroids
- Tadalafil
- Vitamin A derivatives
3. What medication may have predisposed the patient to developing his current condition? 3. Tadalafil
Phosphodiesterase-5 inhibitors (PDE5i) are used for the treatment of erectile dysfunction and pulmonary arterial hypertension and have been associated with NAION. These drugs include sildenafil (Viagra), cardenafil (Levitra), tadalafil (Cialis) and avanafil (Stednra). Pfizer performed a case-crossover retrospective study and an odds ratio of 2.15 was calculated for developing definite NAION the day after exposure to a PDE5i. If the patient used any of these drugs it would increase the index of suspicion for NAION. If the patient is diagnosed with NAION, he would need to be counselled on the increased risk of developing NAION in the other eye if continues to use this medication.
4. What is the next most appropriate course of action for this patient?
- Admission to hospital for a stroke workup (MRI of the brain, MRA of the head and neck, ECHO, and Holter monitor)
- MRI of the brain and orbits with contrast
- Acute reduction in blood pressure
- Inflammatory blood markers
- None of the above
4. What is the most appropriate course of action for this patient? 4. Inflammatory blood markers
The patient’s presentation of sudden painless vision loss from an optic neuropathy with optic disc edema is most consistent with a right anterior ischemic optic neuropathy (AION). The presence of vascular risk factors, a disc-at-risk in the left eye, and the absence of any systemic symptoms of giant cell arteritis is highly suggestive of NAION. The most important next step in a patient with AION above 50 years of age is evaluation for the arteritic form of the disease. Arteritis means related to a vasculitis such as GCA, which affects large and medium-sized blood vessels. Evaluation for GCA involves a thorough history to determine the presence of systemic symptoms, examining the patient for signs that would suggest more diffuse ischemia (such as cotton wool spots away from the nerve) and obtaining blood inflammatory markers, specifically a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). The absence of systemic symptoms of GCA such as headache, jaw claudication and scalp tenderness does not rule out the diagnosis and bloodwork (CBC, ESR and CRP) is usually obtained for every patient over 50 years of age. The CBC, ESR, and CRP must be interpreted in the context of the patients systemic health and the pre-test probability of GCA. Admission for a stroke workup is not required since the pathophysiology of NAION is different from an ischemic stroke. NAION is thought to be due to transient hypoperfusion of the optic nerve head and does not involve embolic infarction due to the small size and architecture of the blood vessels supplying this region of the optic nerve.
Clinical Pearl
The most important step in evaluating a patient with an anterior ischemic optic neuropathy over 50 years of age is to exclude giant cell arteritis with a thorough history, examination, and bloodwork that includes a platelet count, ESR, and CRP. A temporal artery biopsy may be necessary.
The results of the bloodwork are shown below:
Hemoglobin 142 g/L (normal 135-175g/L)
WBC 8.0 x 109/L (normal 4.0-11.0 x 109/L)
Platelets 352 x 109/L (normal 150-400 x 109/L)
ESR 2 mm/h (normal age/2)
CRP 1 mg/L (normal <5 mg/L)
His inflammatory markers were normal and a diagnosis of NAION was made
5. What treatment for NAION is supported by prospective randomized controlled trials?
- Intravenous methylprednisolone 1 g daily for 3 days
- Oral prednisone
- Carotid endarterectomy
- None
5. What treatment for NAION is supported by prospective randomized controlled trials? 4. None
There is no treatment for NAION supported by prospective, randomized trials. Oral steroids have been proposed, but this is based on a nonrandomized, retrospective study that has been criticized for methodological design issues. Since there are no symptoms or signs of GCA and the inflammatory markers are normal, steroids are not recommended. In a patient with vascular risk factors, a low-dose aspirin may be recommended to reduce the chance of fellow eye involvement, although there is no strong evidence for this recommendation.
6. Why are the majority of people with NAION white?
- Whites tend to have smaller cup-to-disc ratios than blacks
- Whites tend to have more vascular risk factors than blacks
- Whites tend to treat their blood pressure more aggressively
- Whites tend to have smaller axial lengths
6. Why are the majority of people with NAION white? 1. Whites tend to have smaller cup-to-disc ratios than blacks
A disc-at-risk is essential for the development of NAION and its absence should raise the possibility of another diagnosis. Blacks tend to have larger cup-to-disc ratios than whites and are therefore less likely to have a disc-at-risk and NAION.
7. Which of the following is a risk factor for NAION?
- Young age
- Obstructive sleep apnea
- Use of anticoagulation
- Liver disease
7. Which of the following is a risk factor for NAION? 2. Obstructive sleep apnea
The most common systemic risk factors for NAION include hypertension (present in about 50% of patients) and diabetes (present in about 25% of patients). Obstructive sleep apnea is also a strong independent risk factor for NAION and a systematic review and meta-analysis found a pooled odds ratio of developing NAION of 6.18 (95% CI, 2.00-19.11) from four prospective cohort studies and one case-control study. It is important to ask for symptoms of obstructive sleep apnea (eg. daytime sleepiness, restless sleep, loud snoring) in patients with NAION and refer the patient to their primary care provider or a sleep specialist if this is a concern. Other risk factors associated with NAION include hypercholesterolemia, ischemic heart disease, tobacco use, and systemic atherosclerosis, although there are few rigorous population-based studies establishing these associations.
8. How long does the disc edema typically persist in NAION?
- 2-4 weeks
- 6-11 weeks
- 12-18 weeks
- Usually persists up to 12 months
8. How long does the disc edema typically persist in NAION? 2. 6-11 weeks
Previous studies have found that the median time (25th-75th percentile) to spontaneous resolution of optic disc edema in NAION was 7.9 (5.8-11.4) weeks. The time to resolution of optic disc edema was longer in diabetics, but shorter in patients with worse visual field defects and worse visual acuity. If the disc edema persists longer than expected, other diagnoses such as a compressive optic neuropathy from a retrobulbar mass should be considered.
9. What does the optic nerve look like after the disc edema resolves?
- The optic nerve returns to its appearance before the onset of edema
- The optic nerve becomes very cupped
- The optic nerve becomes very cupped and pale
- The optic nerve becomes pale
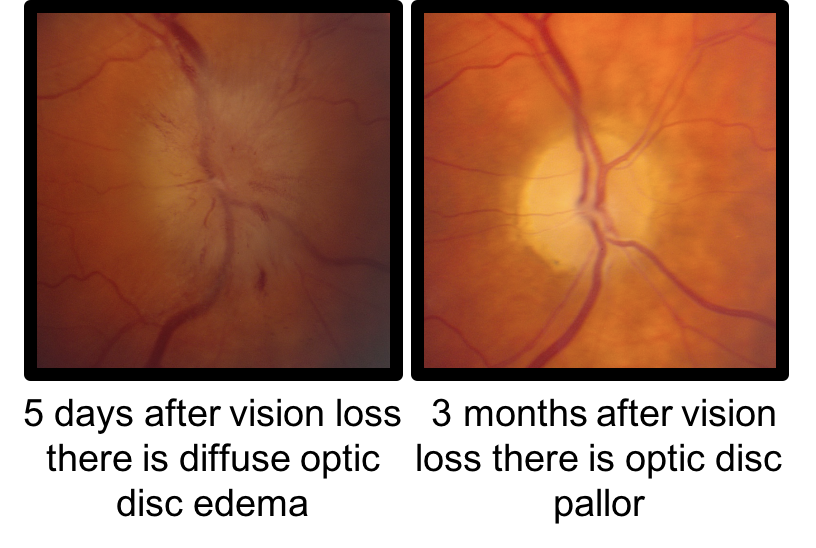
9. What does the optic nerve look like after the disc edema resolves? 4. The optic nerve becomes pale
After the disc edema resolves the optic nerve becomes pale due to the loss of ganglion cell axons. Significant cupping does not typically develop in patients with NAION after the disc edema resolves unlike the arteritic form associated with GCA, which is associated with both cupping and pallor of the optic nerve.
10. What approximate percentage of patients with NAION have ocular pain at presentation?
- 10%
- 25%
- 50%
- 72%
10. What approximate percentage of patients with NAION have ocular pain? 1. 10%
Ocular pain is a characteristic finding in patients with optic neuritis (92% of patients), but is less likely in NAION (approximately 10-12% of patients). The pain in NAION is usually mild, vague and localizes around the eye. There is considerable overlap between optic neuritis and NAION and the presence of pain may be a useful differentiating factor.
11. What is the 5-year risk of developing NAION in the fellow eye?
- 5%
- 15%
- 25%
- 50%
11. What is the 5-year risk of developing NAION in the fellow eye? 2. 15%
The Ischemic Optic Neuropathy Decompression Trial (IONDT) found that new NAION occurred in the fellow eye in 14.7% of patients during a median follow-up of 5.1 years. A history of diabetes and baseline visual acuity 20/200 or worse were significantly associated with new NAION in the fellow eye.
12. How often does NAION recur in the same eye?
- < 5%
- 10-15%
- 25-30%
- 35-40%
12. How often does NAION recur in the same eye? 1. <5%
NAION recurs in the affected eye less than 5% of the time. This is probably because the optic atrophy that develops relieves the crowding of optic nerve and the patient no longer has a disc-at-risk.
13. What is an MRI of the orbits with contrast and fat suppression expected to show in this patient?
- Enhancement of the intraorbital optic nerve
- Enhancement of the optic nerve sheath
- Enhancement of optic chiasm
- Normal MRI
13. What is an MRI of the orbits with contrast and fat suppression expected to show in this patient? 4. Normal MRI
Enhancement of the optic nerve is assessed on a post-contrast T1 MRI sequence with fat suppression. Fat suppression means that the normally bright orbital fat on a T1 sequence is suppressed so that it appears dark and enhancement of the optic nerve can more easily be seen. Enhancement appears as a bright signal in the optic nerve and is due to breakdown of the blood-optic nerve barrier, primarily seen in inflammatory conditions such as optic neuritis. This allows the gadolinium contrast to leak into the optic nerve. In NAION, the MRI is normal since it is due to a very localized ischemic event at the anterior part of the intraocular optic nerve without breakdown of the blood-optic nerve barrier. Enhancement is a useful way of differentiating optic neuritis from NAION as shown below.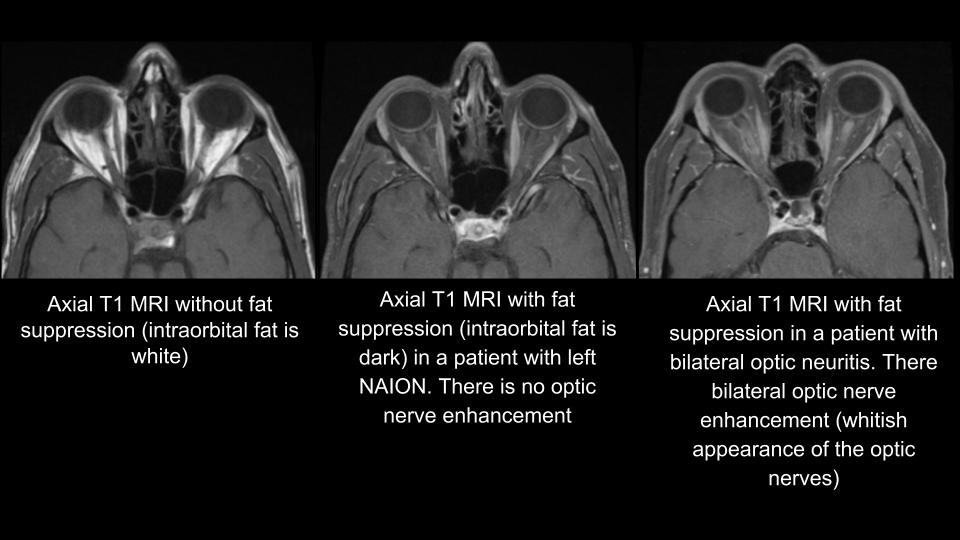
14. What finding on clinical examination would increase the likelihood of giant cell arteritis in a patient with an anterior ischemic optic neuropathy?
- Chalky white optic disc edema
- Cotton wool spots away from the optic disc
- Delayed choroidal filling seen on indocyanine green angiography
- A large cup-to-disc ratio in the fellow eye
- All of the above
14. What finding on clinical examination would increase the likelihood of giant cell arteritis in a patient with an anterior ischemic optic neuropathy? 5. All of the above
The optic disc is usually hyperemic in NAION compared to AAION, which is usually chalky white due to more severe infarction. Cotton wool spots away from the disc and delayed choroidal filling suggest more diffuse ischemia than that isolated to the optic nerve, which is also more suggestive of GCA. If there is a normal or large cup-to-disc ratio in the fellow eye, the diagnosis of NAION must be reconsidered. 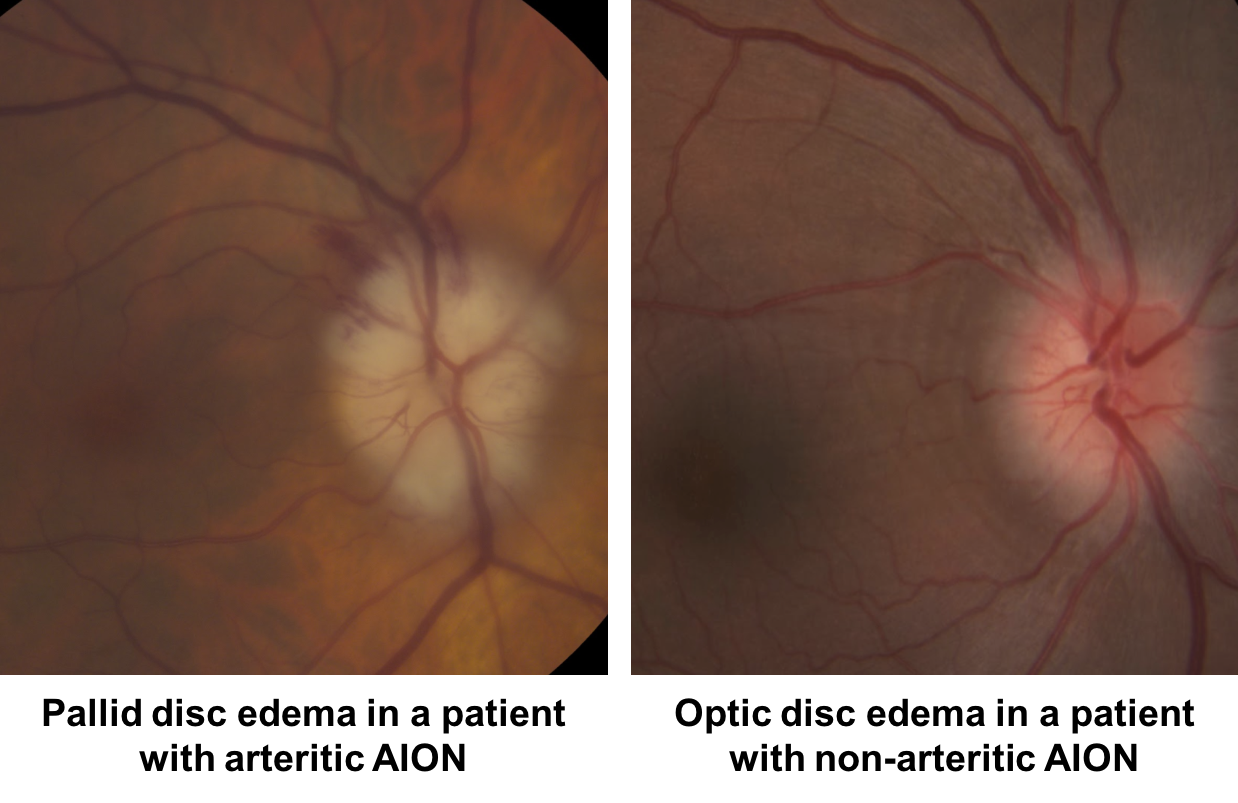
15. What is the natural history of NAION?
- Complete recovery of vision within 3 months
- Complete recovery of vision within 6-8 months
- Mild or no improvement in vision
- Continued worsening of vision for up to 6 months
15. What is the natural history of NAION? 3. Mild or no improvement in vision
Most patients with NAION have mild or no improvement in their vision. The IONDT found that 42.7% of patients with NAION and vision worse than 20/60 had an improvement of their visual acuity by 3 or more lines at 6 months. Some of this improvement may be due to changes in fixation strategy as patients learn to better use the area of normal visual field. Complete recovery of vision is extremely unusual and if this occurs, other diagnoses such as optic neuritis should be considered.
16. What medication has been associated with an optic neuropathy that resembles NAION?
- Tetracycline
- Amiodarone
- Nifedipine
- Digoxin
16. What medication has been associated with an optic neuropathy that resembles NAION? 2. Amiodarone
Amiodarone has been associated with an optic neuropathy that resembles NAION and some have argued that NAION and amiodarone-optic neuropathy are not distinct entities. This is mainly because both groups of patients share similar vascular risk factors. However, histopathologic studies have shown lysosome-like intracytoplasmic membranous lamellar bodies accumulated in large optic nerve axons in patients on amiodarone. These may decrease or block axoplasmic flow leading to optic disc edema. In addition, amiodarone-associated optic neuropathy has been reported to have a more insidious onset, slower progression, protracted disc swelling and often involve both eyes, suggesting that it is different from a typical NAION.
17. Can asymptomatic optic disc edema precede vision loss in NAION?
- No, all cases with optic disc edema have vision loss
- No, only cases related to giant cell arteritis may have asymptomatic optic disc edema
- Yes, some cases may present with asymptomatic optic disc edema
- Yes, but only if the patient is diabetic
17. Can asymptomatic optic disc edema precede vision loss in NAION? 3. Yes, some cases may present with asymptomatic optic disc edema
Some patients that develop NAION have been noted to have optic disc edema that precedes vision loss. This has been termed “incipient NAION” or “pre-symptomatic NAION”. In a previous study of 54 patients with incipient NAION, 25% went on to develop classic NAION and 20% developed classic NAION after the disc edema resolved. Incipient NAION is similar to what has been reported as “diabetic papillopathy” in that there is relatively preserved visual function in the presence of optic disc edema in patients with vascular risk factors and a disc-at-risk. There is likely a spectrum of ischemia that ranges from asymptomatic, pre-infarct edema with a low level of ischemia to the typical NAION case with irreversible vision loss and more severe infarction. Patients with unilateral asymptomatic optic disc edema should be investigated for other causes of asymptomatic disc edema such as an optic nerve sheath meningioma even if there is a disc-at-risk in the fellow eye.
18. The presence of which ocular condition may increase the risk of NAION?
- Optic disc drusen
- Optic nerve pit
- Optic nerve coloboma
- Age-related macular degeneration
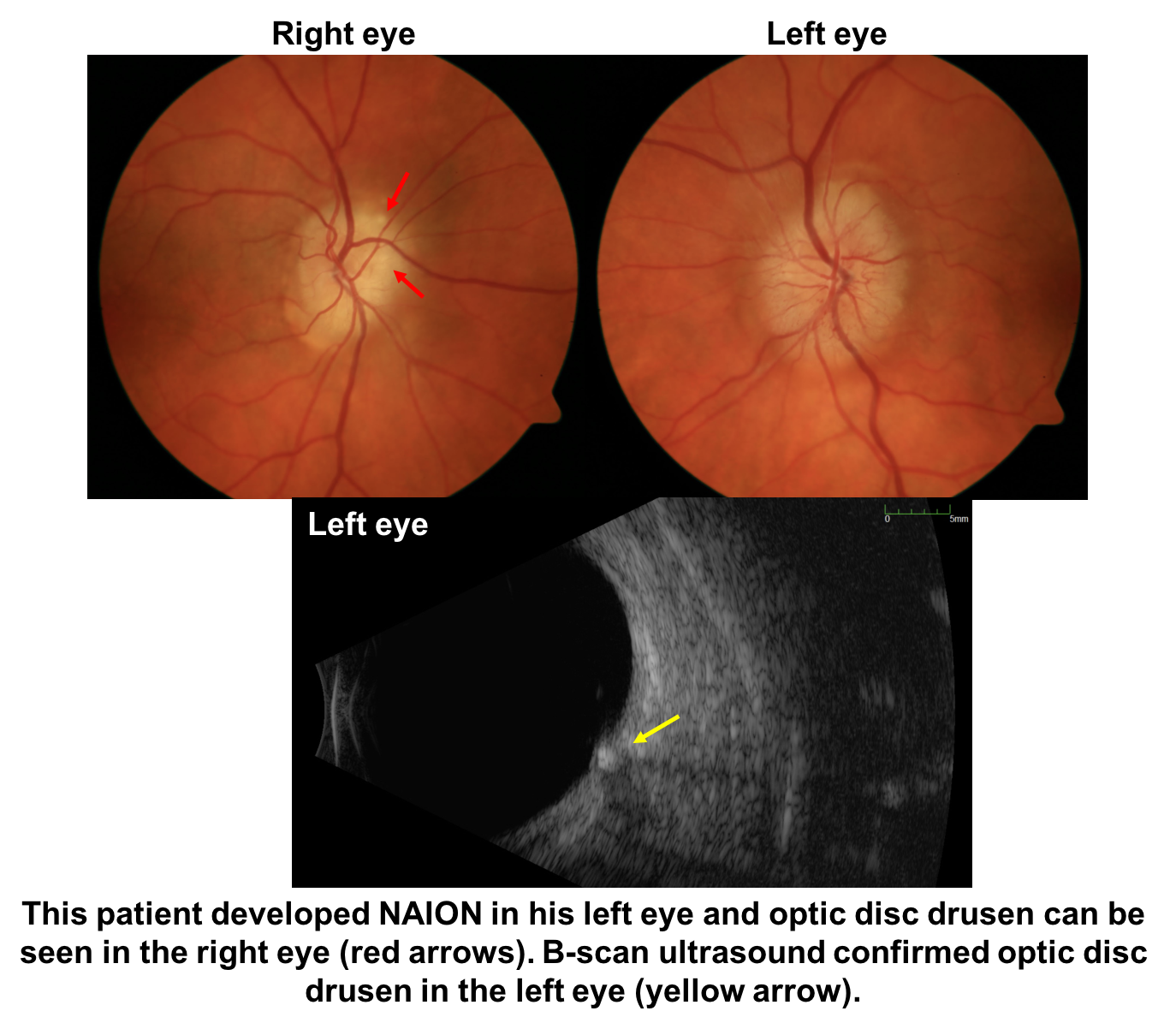
18. The presence of which ocular condition may increase the risk of NAION? 1. Optic disc drusen
Optic disc drusen are abnormal deposits of protein-like material in the optic disc. Since these deposits create a more congested optic nerve head, like a disc-at-risk, they may predispose to the development of NAION. A previous study on the relationship between NAION and optic disc drusen found that patients with NAION associated with disc drusen were younger, but shared similar vascular risk factors and clinical features to those with NAION without drusen.
19.A 60-year-old patient with hypertension suddenly lost vision in his left eye 6 months ago, but has not seen an eye doctor since that time. He has a disc-at-risk in the right eye and a left optic neuropathy with optic disc pallor. What is the next most appropriate course of action?
- Observation and optimization of vascular risk factors
- Low-dose aspirin
- MRI of the brain and orbits with contrast
- Temporal artery biopsy
19. A 60-year-old patient with hypertension suddenly lost vision in his left eye 6 months ago, but has not seen an eye doctor since that time. He has a disc-at-risk in the right eye and a left optic neuropathy with optic disc pallor. What is the next most appropriate course of action? 3. MRI of the brain and orbits with contrast
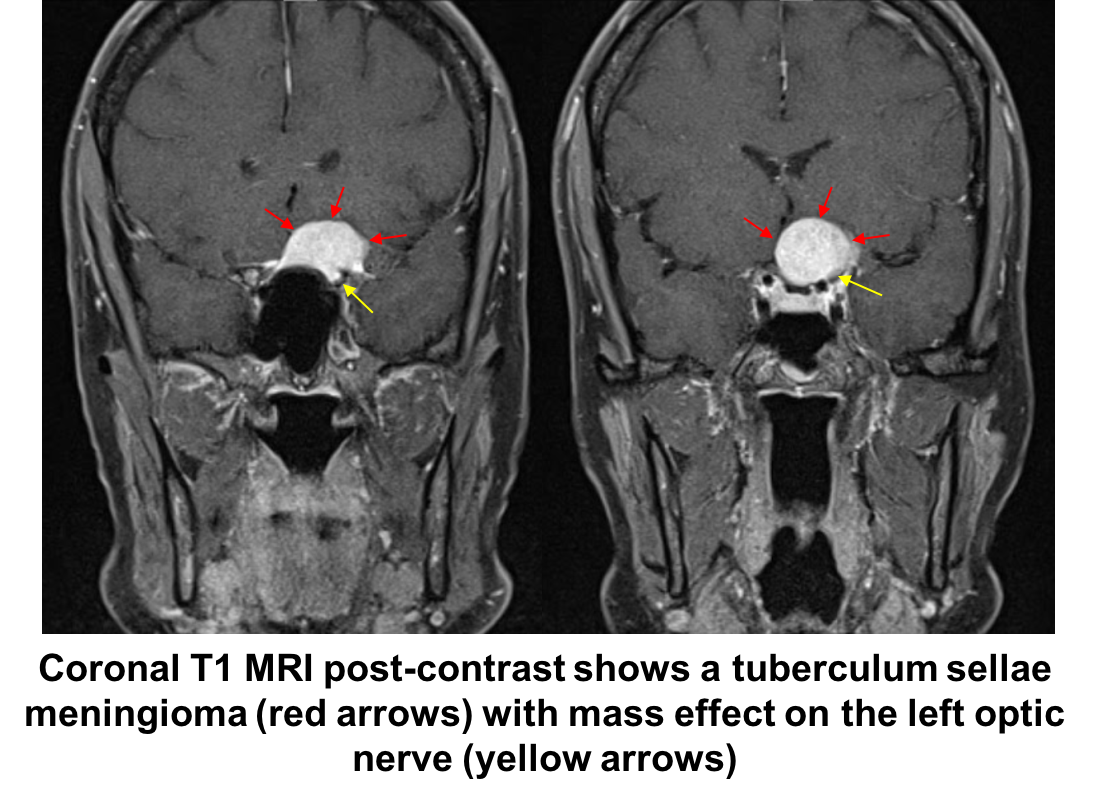
Although this patient has vascular risk factors, a disc-at-risk in this right eye and a left optic neuropathy, left optic disc edema has not been observed, which may simply be because he did not see an eye doctor in the acute period. Although his vision loss may be due to a left NAION, an MRI of the brain and orbits with contrast should be performed to assess for a compressive lesion. NAION should not be assumed without documented optic disc edema. Compressive optic neuropathies usually present with gradual loss of vision, but may sometimes present with acute vision loss or an acute awareness of vision loss if the fellow eye is covered by the patient. This patient had a left compressive optic neuropathy from a tuberculum sellae meningioma (shown below).
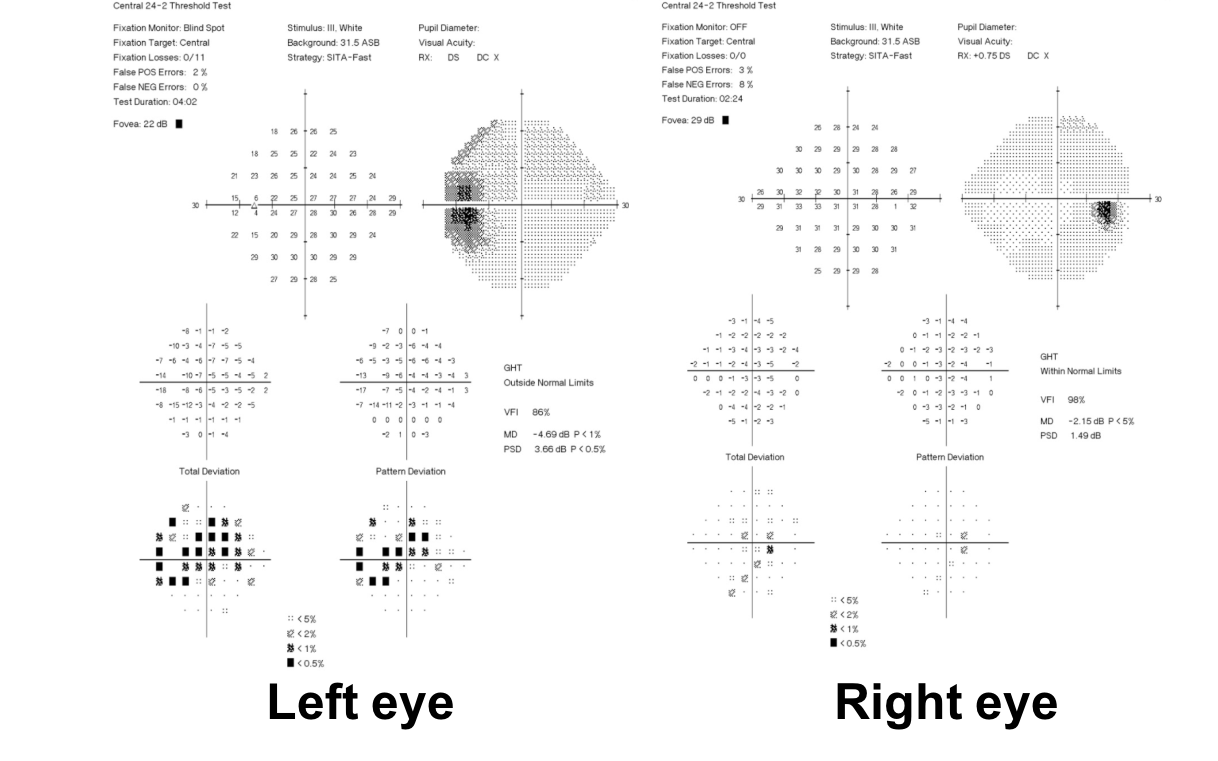
20. A 64 year old man is referred for left eye painless vision loss that occurred 2 days ago. His visual acuity is 20/20 OD and 20/100 OS. Optic disc photographs and Humphrey visual fields are shown below. What is the next most appropriate step in the care of this patient?
- CBC, ESR, and CRP
- MRI of the brain and orbits with contrast
- CTA of the head and neck
- OCT of the macula
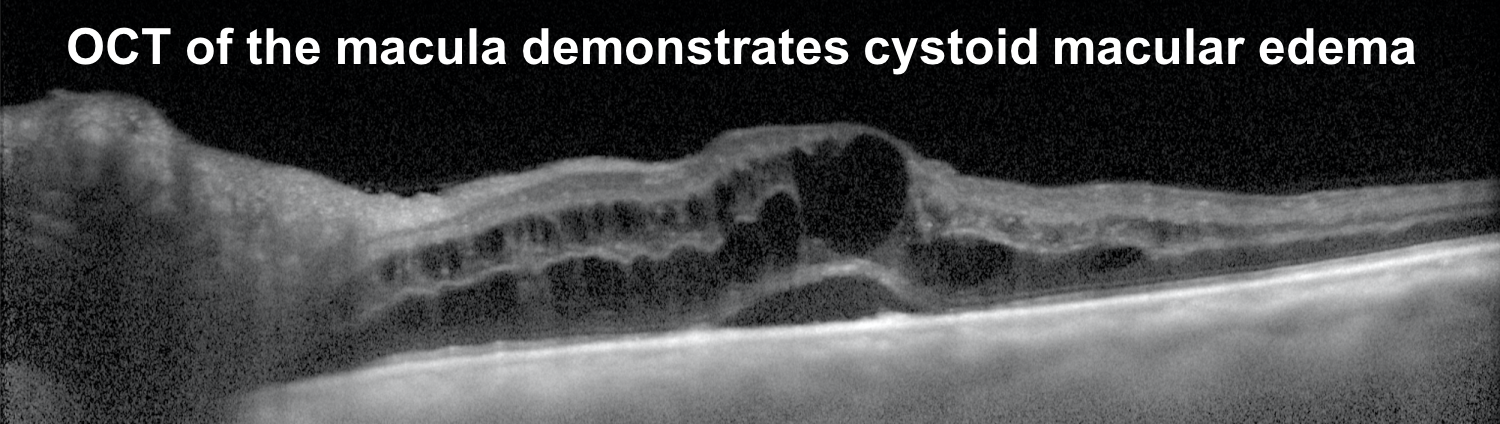
20. A 64-year-old man is referred for left eye painless vision loss that occurred 2 days ago. His visual acuity is 20/20 OD and 20/100 OS. Optic disc photographs and Humphrey visual fields are shown below. What is the next most appropriate step in the care of this patient? 4. OCT of the macula
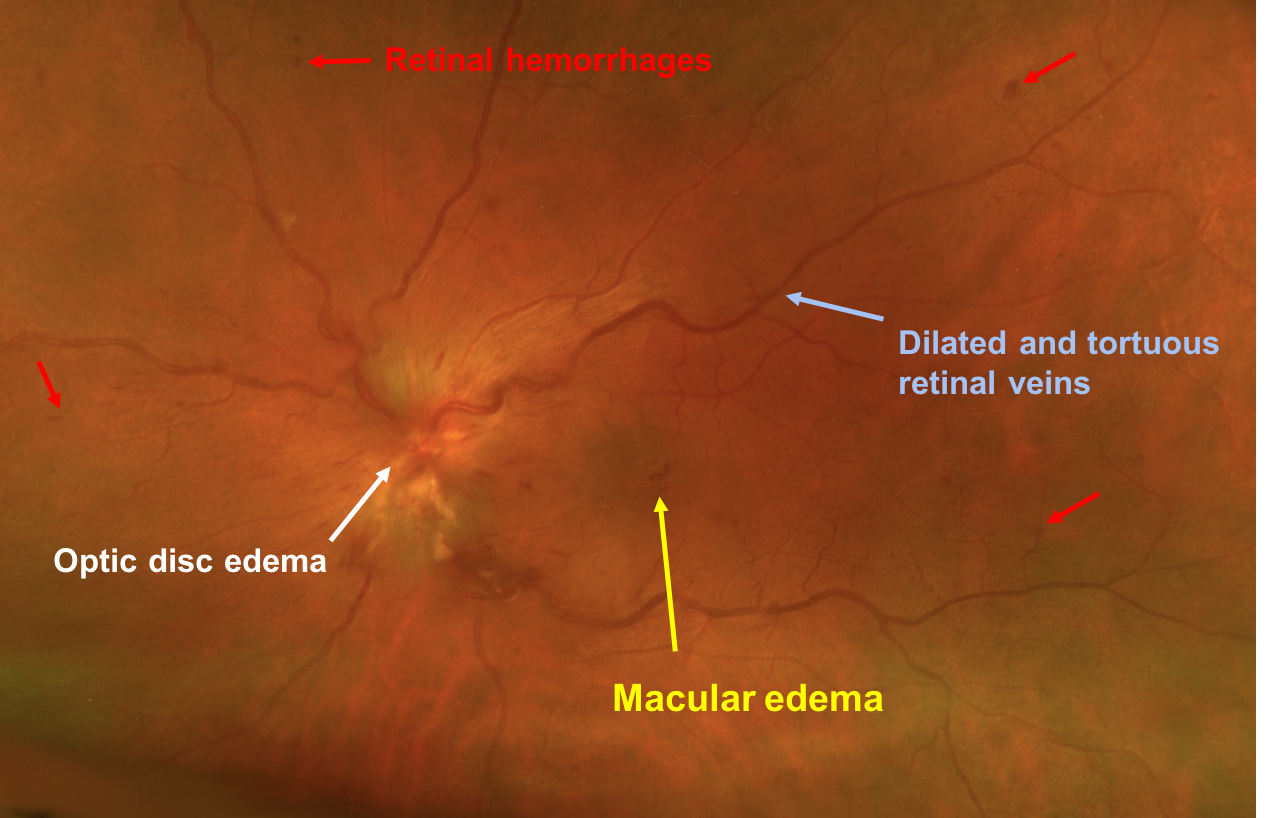
This patient has optic disc edema, peripapillary hemorrhages, cotton wool spots, and most importantly, dilated and tortuous retinal veins in the left eye. The diagnosis is left central retinal vein occlusion (CRVO) and this patient should have an OCT of the macula to assess for macular edema. CRVOs are categorized as ischemic if they have at least 10 disc areas of retinal capillary nonperfusion. Ischemic cases tend to have poor vision, an RAPD, and a dense central scotoma. The optic disc edema tends to be more severe and persist longer in patients with ischemic CRVOs with a median time to resolution of 21.7 months compared to 9.8 months in non-ischemic cases. An Optos photo and Spectralis macular OCT of the left eye are shown below. This is unlikely to be NAION given the changes in the retinal veins and the absence of a disc-at-risk in the right eye.
Case Summary
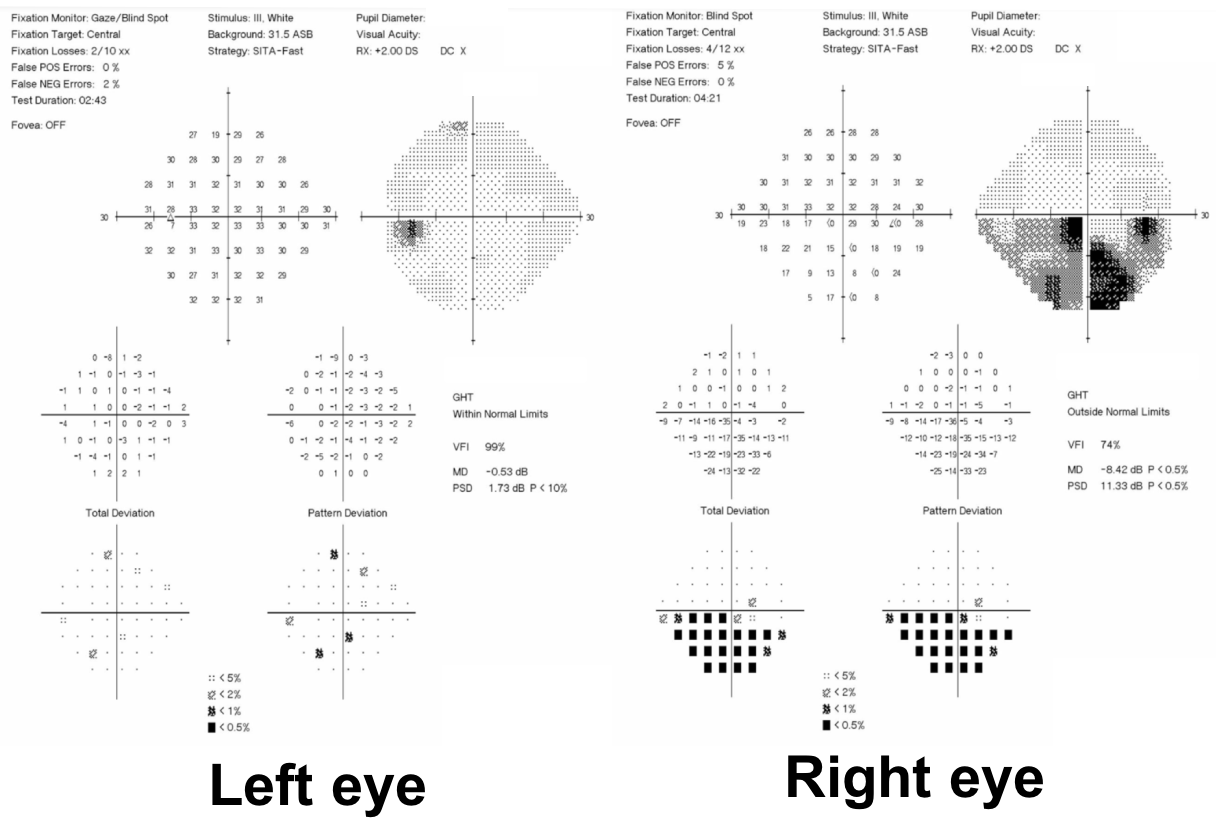
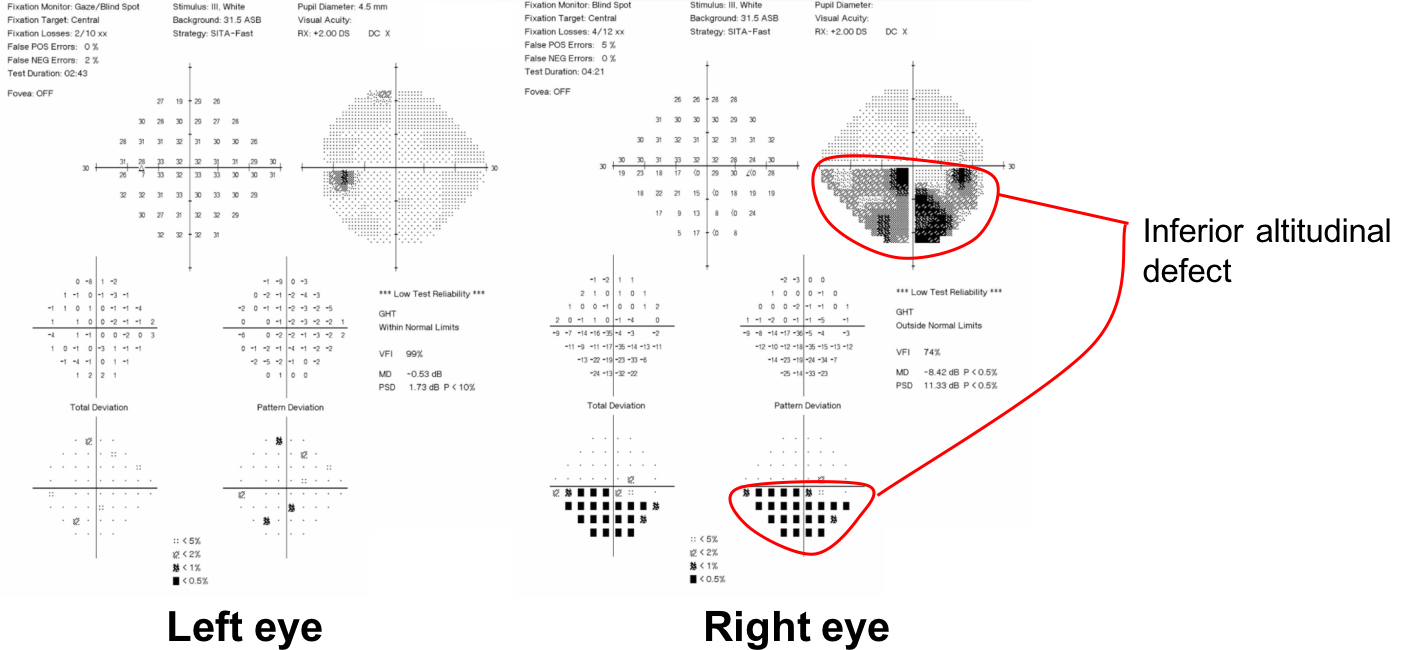
He presented with sudden painless vision loss and had signs of a right anterior optic neuropathy, including a right RAPD, inferior altitudinal visual field defect and optic disc edema. The presence of vascular risk factors and left disc-at-risk were highly suggestive of NAION. There were no signs or symptoms of giant cell arteritis including normal inflammatory blood markers. His visual field remained stable and his optic disc edema resolved after 10 weeks, consistent with the expected evolution of NAION.
Further reading:
- Biousse V, Newman NJ. Ischemic optic neuropathies. New Engl J Med 2015;372:2428-36. http://www.nejm.org/doi/full/10.1056/NEJMra1413352
-
Pomeranz, HD. Erectile dysfunction agents and nonarteritic anterior ischemic optic neuropathy. Neurol Clin 2017;35:17-27. https://www.ncbi.nlm.nih.gov/pubmed/27886893
-
Hayreh SS, Zimmerman MB. Optic disc edema in non-arteritic anterior ischemic optic neuropathy. Graefe’s Arch Clin Exp Ophthalmol 2007;245:1107-1121. https://www.ncbi.nlm.nih.gov/pubmed/17219123
-
Swartz NG, Beck RW, Savino PJ, et al. Pain in anterior ischemic optic neuropathy. J Neuroophthalmol 1995;15(1):9-10. https://www.ncbi.nlm.nih.gov/pubmed/7780575
-
Newman NJ, Scherer R, Langenberg P, et al. The fellow eye in NAION: Report from the ischemic optic neuropathy decompression trial follow-up study. Am J Ophthalmol 2002;134(3):317-28. https://www.ncbi.nlm.nih.gov/pubmed/12208242
-
The Ischemic Optic Neuropathy Decompression Trial Research Grop. Optic nerve decompression surgery for nonartertic ischemic optic neuropathy (NAION) is not effective and may be harmful. JAMA 1995;273:625-632. https://www.ncbi.nlm.nih.gov/pubmed/7844872
-
Wang AG, Cheng HC. Amiodarone-associated optic neuropathy: clinical review. Neuroophthalmology 2016;41(2):55-58. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5354097/
-
Arnold AC. The 14th Hoyt lecture: Ischemic optic neuropathy: the evolving profile, 1966-2015. J Neuroophthalmol 2016;36:208-215. https://www.ncbi.nlm.nih.gov/pubmed/27176556
-
Hayreh SS, Zimmerman MB. Incipient nonarteritic anterior ischemic optic neuropathy. Ophthalmology 2007;114:1763-1772. https://www.ncbi.nlm.nih.gov/pubmed/17391767
-
Wu Y, Zhou LM, Lou H, et al. The association between obstructive sleep apnea and nonarteritic anterior ischemic optic neuropathy: a systematic review and meta-analysis. Curr Eye Res 2016;41(7):987-92. https://www.tandfonline.com/doi/abs/10.3109/02713683.2015.1075221